

Introduction: Two Sexual Disorders, One Clinical Problem
Erectile dysfunction (ED) and premature ejaculation (PE) are often treated as separate complaints—two boxes on a problem list, two prescriptions, and ideally two quick wins. In real life, they behave more like an intertwined system. ED increases performance anxiety, which accelerates ejaculation. PE increases fear of failure, which worsens erection quality. Patients may not describe this as “bidirectional comorbidity,” of course. They describe it as frustration, avoidance, and a growing sense that sex has become a test they keep failing.
The comorbidity is common and clinically consequential. When ED and PE coexist, treating only one condition may not restore sexual satisfaction for the couple. It may improve one metric while leaving the experience unchanged. A man who can achieve a better erection but still ejaculates within seconds does not necessarily feel “treated.” His partner often agrees, quietly and decisively.
This is why combination strategies deserve serious attention. The challenge is finding combinations that are not only effective, but practical. In sexual medicine, practicality is not a secondary detail—it is the difference between a therapy that is used and one that is abandoned.
A randomized controlled trial evaluated an approach built for real-world behavior: on-demand tadalafil 20 mg (for erection quality) combined with topical lidocaine spray (for ejaculatory control). The logic is simple: tadalafil offers systemic vascular support with a predictable onset, while lidocaine acts locally within minutes. The question is whether that logic translates into measurable outcomes for men who have both ED and PE—and whether it does so without adding new safety problems.
The Biological Logic: Why One Drug Is Usually Not Enough
ED and PE share psychological and neurobiological links, but their core mechanisms differ. ED is often driven by impaired penile hemodynamics, endothelial dysfunction, autonomic imbalance, or medication effects. PE—especially lifelong PE—frequently involves heightened penile sensitivity, altered serotonergic signaling, or learned behavioral patterns reinforced over years.
A PDE5 inhibitor such as tadalafil improves erection quality mainly by enhancing nitric oxide–cGMP signaling, increasing smooth muscle relaxation, and supporting penile blood flow. That can indirectly affect PE by reducing anxiety and improving confidence, but it does not directly reduce penile sensitivity or strengthen ejaculatory control. For many men with comorbid PE, “less anxiety” is helpful but insufficient. A stopwatch does not negotiate.
Topical anesthetics, in contrast, target one of the most practical contributors to PE: penile hypersensitivity. Lidocaine reduces sensory input, raising the threshold required to trigger ejaculation. When used correctly, it can prolong intravaginal ejaculatory latency time (IELT) and improve perceived control. Its main drawbacks are localized numbness, possible transfer to the partner, and reduced sensation if overdosed.
The combination approach therefore fits the comorbidity structure: systemic support for erection plus local modulation of sensitivity. It aims to treat both disorders at the level where they actually operate, rather than hoping one therapy will accidentally solve both.
Study Design: Pragmatic Randomization With Clear Endpoints
The study enrolled men with comorbid ED and PE and randomized them into two groups for 12 weeks. One group used on-demand tadalafil 20 mg alone, taken 30 minutes before intercourse. The other group used the same tadalafil regimen but added lidocaine spray applied 5 minutes before intercourse.
This timing matters. Many combination regimens in sexual medicine fail not because they are ineffective, but because their timing is unrealistic. Some oral PE therapies require longer lead times or have side-effect profiles that make continued use unlikely. By selecting a fast-acting topical agent, the protocol was designed around what couples can plausibly do without turning intimacy into a medication choreography.
The study measured outcomes that reflect both physiology and lived experience:
- IIEF-5 for erectile function
- CIPE-5 for premature ejaculation symptoms (a validated Chinese index assessing control, satisfaction, latency, partner satisfaction, and anxiety)
- IELT measured with the stopwatch method
- Sexual Satisfaction Score (SSS) for both patient and spouse
Safety outcomes included adverse event incidence and specific symptoms such as headache, flushing, nasal congestion, fatigue, nausea/vomiting, and dyspepsia.
Results: Erection Improves in Both Groups, Ejaculation Improves Only With Lidocaine
The most clinically important result is also the simplest: tadalafil improves erectile function, but tadalafil alone does not reliably treat PE in men who have both disorders.
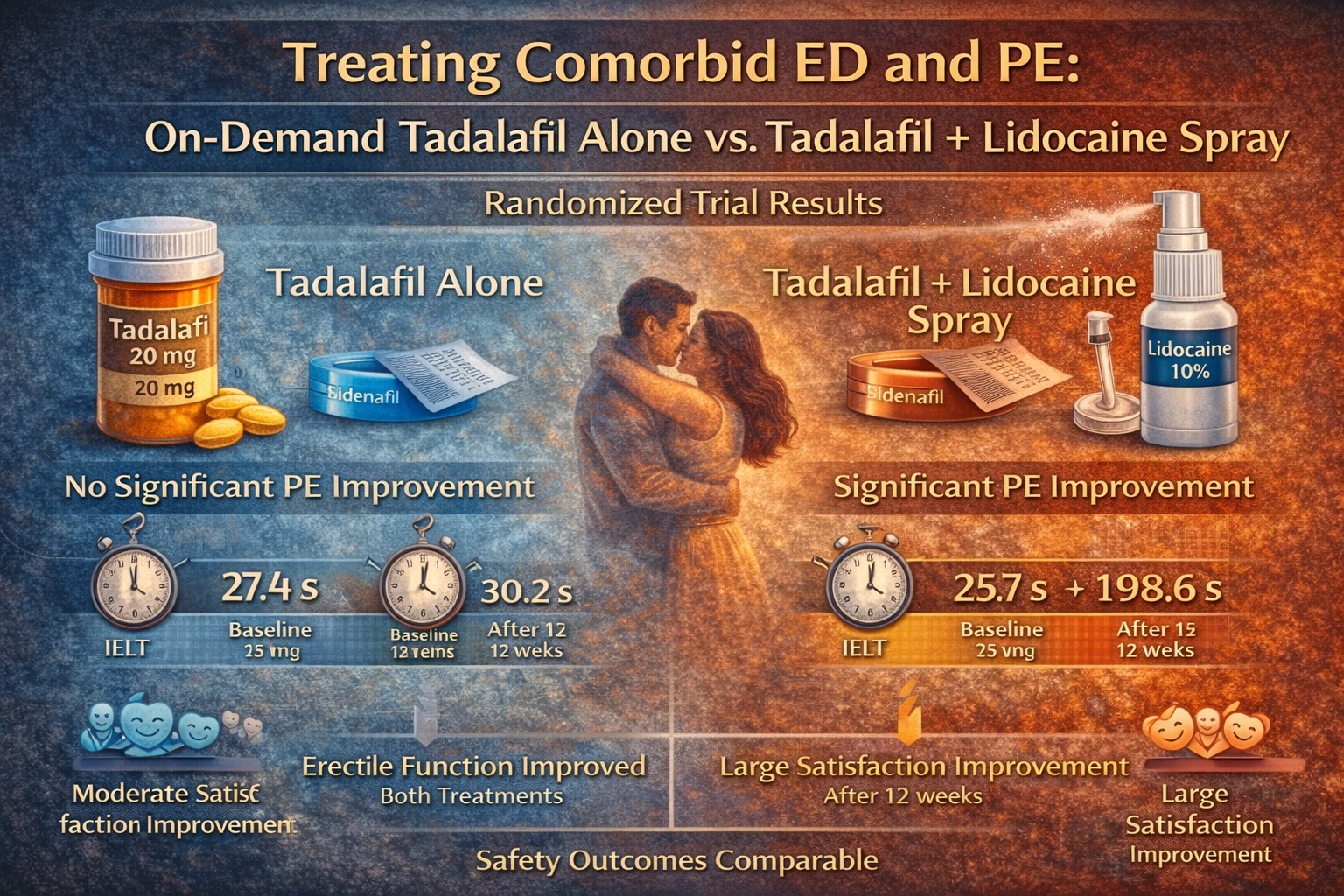
Both groups improved their IIEF-5 scores significantly over 12 weeks, and the difference between groups was not statistically significant. This indicates that adding lidocaine did not compromise erectile benefits, which is essential. In sexual medicine, therapies that improve one outcome by damaging another are common—and deeply unpopular.
The PE outcomes, however, separated the groups sharply. The combination group showed significant improvement in CIPE-5 scores, whereas the tadalafil-only group did not achieve significant change. The IELT findings were even more striking: in the combination group, IELT increased from about 25.7 seconds at baseline to approximately 198.6 seconds after treatment—an improvement that is clinically meaningful, not merely statistically pleasant. Meanwhile, the tadalafil-only group showed no significant IELT change (roughly 27.4 seconds to 30.2 seconds).
Sexual satisfaction followed the same pattern. Satisfaction scores improved markedly for both patients and spouses in the combination group, while changes were minimal and non-significant with tadalafil alone. That spouse outcome matters more than many clinicians admit. A couple’s sexual health is a two-person system; treating one person’s score while ignoring the shared experience is a reliable way to produce “successful therapy” and an unhappy home.
Why Sexual Satisfaction Changes Are the Real Headline
Clinicians are trained to respect objective endpoints: scores, latency times, p-values. Patients care about a different endpoint: whether sex feels normal again. Satisfaction is the closest proxy to that reality.
The satisfaction improvement in the combination group was substantial in both patient and spouse measures. This suggests that prolonging IELT did not merely delay ejaculation in a mechanical sense; it likely improved perceived control, reduced anxiety, and allowed a more natural sexual sequence. In other words, it restored a narrative of intimacy rather than a race against time.
This is where a little clinical irony belongs. We often assume that “erection = sex solved.” The data here remind us that this belief is as medically inaccurate as it is emotionally naïve. For men with comorbid ED and PE, improving erection without addressing ejaculation may simply create a better-quality version of the same frustrating event.
By treating both components—rigidity and timing—the combination therapy seems to produce what patients actually want: improved confidence, improved partner experience, and less avoidance.
Safety: Comparable Adverse Event Rates With an Important Practical Caveat
The overall incidence of adverse events was similar between groups, with no statistically significant difference. The types of adverse events reported were familiar for tadalafil-based therapy: headache, flushing, nasal congestion, fatigue, gastrointestinal discomfort.
This is reassuring because combination therapy often triggers legitimate safety worries. The study suggests that adding topical lidocaine, at least in the described regimen, does not meaningfully increase systemic side effects.
However, topical therapy brings a different kind of risk: misuse. Lidocaine spray is effective, but it has a narrow “sweet spot” between “enough to help” and “so much that sensation collapses.” The study’s authors addressed this directly by providing detailed usage guidance: waiting time after spraying, avoiding urethral application, recommendations around condom use to prevent partner transfer, and warnings about overdosing that can cause excessive numbness and delayed or absent ejaculation.
This is not decorative advice—it is the difference between a successful intervention and a self-inflicted problem. If clinicians use this approach, patient instruction must be part of the prescription.
Practical Clinical Guidance: How to Use This Evidence at the Bedside
This trial supports a clinically intuitive strategy: in comorbid ED + PE, treat both domains directly rather than expecting ED therapy to magically solve ejaculatory control. The approach is especially relevant in patients whose PE remains severe despite improved erections.
In practice, tadalafil on demand is often chosen for its flexibility and familiarity, while lidocaine offers immediate PE control without the systemic side effects or discontinuation patterns seen with some oral PE agents. The combination also allows timing compatibility: tadalafil 30 minutes before, lidocaine 5 minutes before.
If a clinician adopts this strategy, three themes should guide implementation: selection, instruction, and follow-up. Selection means confirming true comorbidity and excluding conditions where topical agents could be problematic or where partner irritation risk is high. Instruction means explicit application technique and partner-protection steps. Follow-up means reassessing satisfaction, IELT, and side effects, and adjusting dose/exposure rather than abandoning the plan prematurely.
One practical advantage is that this regimen is inherently modular. If erection improves but numbness is excessive, lidocaine can be reduced. If PE improves but erection remains inconsistent, tadalafil use can be optimized. That flexibility is valuable in sexual medicine, where a “perfect first regimen” is rare.
Limitations: What the Study Cannot Promise Yet
The study had a modest sample size and was conducted in a single center, which may limit generalizability. Follow-up was 12 weeks, which is enough to demonstrate short-term efficacy but not enough to fully capture long-term adherence, relationship impact, or whether technique quality remains stable over time.
Satisfaction scores and IELT measurements, while clinically meaningful, carry inherent subjectivity and potential bias. Stopwatch IELT is more objective than recall, but it still depends on consistent measurement behavior—something that varies between couples.
Finally, the exclusion criteria removed several comorbid conditions that are common in real ED populations (such as certain chronic pelvic pain conditions or significant psychiatric medication use). In everyday practice, many patients will be more complex than the trial participants.
Despite these limitations, the core signal is strong: for men with both ED and PE, tadalafil alone is often insufficient for PE outcomes, while tadalafil plus lidocaine meaningfully improves ejaculatory control and couple satisfaction without worsening overall safety.
Conclusion: Treat the Couple’s Problem, Not Just the Patient’s Symptom
Comorbid ED and PE should be treated as a linked clinical condition, not as two independent complaints competing for attention. This randomized trial suggests that on-demand tadalafil improves erectile function reliably in these patients, but meaningful improvement in PE symptoms, IELT, and sexual satisfaction requires a targeted PE strategy.
Adding lidocaine spray—a fast-acting, localized intervention—appears to deliver that missing component. The combination produced a large increase in IELT and significant improvements in both patient and partner satisfaction, while maintaining a safety profile comparable to tadalafil alone.
The deeper lesson is that “sexual success” is not a single parameter. It is a shared outcome measured in confidence, control, satisfaction, and the absence of dread. Combination therapy works here because it respects the complexity of the real problem.
FAQ
1. If tadalafil improves erections, why doesn’t it reliably improve premature ejaculation?
Because PE often involves penile hypersensitivity and ejaculatory control pathways that are not directly altered by PDE5 inhibition. Reduced anxiety may help some men, but many require a direct PE treatment.
2. Will lidocaine spray reduce pleasure or cause numbness?
It can—especially if overdosed or applied incorrectly. Used properly, the goal is mild reduction in sensitivity while preserving pleasurable sensation. Technique and dosing matter.
3. Is this combination safe for long-term use?
Short-term safety appears comparable to tadalafil alone in the trial, but longer-term, multicenter studies are still needed. Clinicians should individualize decisions and monitor tolerability and partner effects.
