

The Clinical Problem: Erectile Dysfunction After Prostate Cancer Surgery
Radical prostatectomy remains one of the most effective treatments for localized prostate cancer. Advances in surgical technique—particularly bilateral nerve-sparing radical prostatectomy (nsRP)—have dramatically improved functional outcomes. Yet even in the best hands, erectile dysfunction (ED) remains one of the most distressing and persistent postoperative sequelae.
The paradox is striking. The cancer is removed successfully. The oncologic outcome is excellent. The patient survives—and often lives for decades. But sexual function, a major determinant of quality of life, may not return for 18 months, sometimes longer. In certain men, recovery may extend beyond two years. For some, it never fully recovers.
Phosphodiesterase type 5 inhibitors (PDE5 inhibitors), including tadalafil, have become central to penile rehabilitation strategies. However, one question has remained controversial: does early, continuous tadalafil therapy accelerate true recovery of erectile function, or does it merely provide temporary pharmacologic support?
The randomized trial summarized in the uploaded article provides important answers.
Study Design: A Rigorous Evaluation of Tadalafil After nsRP
The trial was a multicenter, randomized, double-blind, placebo-controlled Phase IV study conducted across nine European countries and Canada. A total of 423 men aged under 68 years who underwent bilateral nerve-sparing radical prostatectomy were randomized into three groups:
- Tadalafil 5 mg once daily (OaD)
- Tadalafil 20 mg on demand (PRN)
- Placebo
Treatment continued for nine months (double-blind treatment phase), followed by a six-week drug-free washout (DFW), and then a three-month open-label once-daily tadalafil phase for all patients.
The key measure of erectile recovery was the International Index of Erectile Function – Erectile Function domain (IIEF-EF). Recovery was defined as an IIEF-EF score ≥22. Importantly, all participants had normal erectile function prior to surgery (IIEF-EF ≥22), ensuring that postoperative dysfunction was surgery-related rather than pre-existing.
The central question was not simply whether tadalafil improved erections during treatment. The deeper and more clinically meaningful question was whether it shortened the time to erectile recovery.
Time to Erectile Function Recovery: The Critical Outcome
The results provide a nuanced but clinically important message.
During the nine-month double-blind treatment phase:
- 29.5% of men on tadalafil once daily achieved IIEF-EF ≥22
- 23.9% on tadalafil PRN achieved this threshold
- 18.4% on placebo achieved recovery
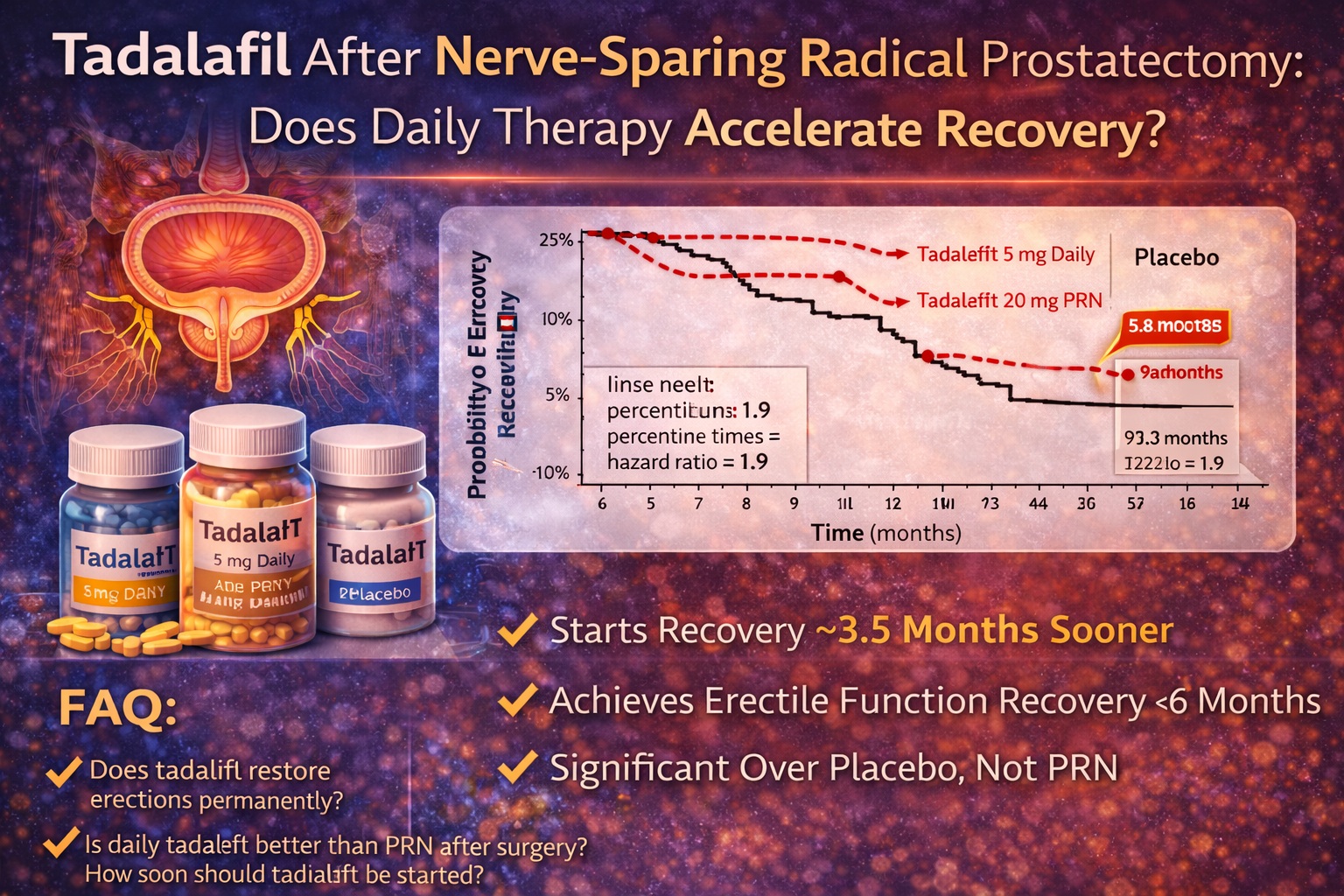
While the raw percentages are modest—no one should pretend otherwise—the Kaplan–Meier time-to-event analysis revealed something more meaningful.
Twenty-five percent of patients reached erectile recovery:
- At 5.8 months with once-daily tadalafil
- At 9.0 months with PRN tadalafil
- At 9.3 months with placebo
This represents a shortening of time to recovery by approximately 3.5 months with daily tadalafil compared to placebo. The hazard ratio for recovery with once-daily tadalafil versus placebo was 1.9 (p = 0.011), indicating nearly double the probability of earlier recovery during treatment.
PRN dosing did not achieve statistical significance.
This distinction between daily and on-demand therapy is clinically crucial.
Why Might Daily Tadalafil Be Different?
Pharmacologically, tadalafil’s long half-life allows for sustained PDE5 inhibition. When administered daily, it reaches steady-state levels. This continuous exposure may produce sustained increases in cavernosal oxygenation, potentially reducing hypoxia-induced fibrosis during the postoperative nerve recovery phase.
Preclinical studies suggest that chronic PDE5 inhibition may:
- Preserve smooth muscle architecture
- Reduce corporal apoptosis
- Maintain endothelial integrity
- Support nitric oxide signaling
After nerve-sparing surgery, neuropraxia and temporary denervation reduce nocturnal erections. Reduced oxygenation leads to fibrosis. Fibrosis reduces elasticity. Elasticity determines function. The cascade is simple—and unforgiving.
Daily tadalafil may interrupt this process by providing ongoing vasodilation and oxygenation, rather than intermittent pharmacologic assistance.
PRN dosing, by contrast, provides episodic support. It improves erections when taken but does not sustain corporal tissue physiology between doses.
In other words, daily tadalafil may serve as rehabilitation, whereas PRN tadalafil functions as episodic assistance.
Clinical Significance Beyond Statistical Significance
Another important measure in the study was the minimally clinically important difference (MCID), defined as a 4-point increase in IIEF-EF score.
In the once-daily tadalafil group, improvement exceeded this clinically meaningful threshold by month five. In the PRN group, this occurred at month nine. In the placebo group, clinically meaningful improvement was delayed further.
This timeline matters. Patients recovering from prostate cancer surgery often experience anxiety, frustration, and concerns about permanent sexual loss. A three-to-four-month acceleration in recovery may have profound psychological and relational impact.
Furthermore, 41% of men in the once-daily tadalafil group improved by at least one ED severity category during treatment, compared to 22.7% in the placebo group.
Even after the six-week drug-free washout, over 75% of those who improved on daily tadalafil maintained at least partial improvement relative to baseline.
This suggests that tadalafil’s effect was not purely symptomatic in all patients.
The Washout Phase: Does Recovery Persist?
After the six-week drug-free washout period, the statistical advantage in full recovery (IIEF-EF ≥22) diminished. This finding is critical.
It indicates that while daily tadalafil accelerated recovery during treatment, unassisted recovery after washout was not significantly different from placebo.
This raises an important interpretive question: does tadalafil accelerate natural recovery, or does it simply maintain function during treatment?
The likely answer is complex.
Nerve regeneration following nsRP can take 18 months or longer. The nine-month double-blind period may have been too short to observe full spontaneous recovery in the placebo group. It remains possible that longer follow-up would demonstrate durable differences.
Indeed, other long-term studies have suggested that early penile rehabilitation may produce superior long-term outcomes, particularly in intermediate-risk patients.
In short: acceleration of recovery is clearly demonstrated; permanent modification of ultimate recovery trajectory remains less certain.
Age and Recovery: Does It Matter?
Interestingly, age group (<61 vs. 61–68 years) did not significantly influence time to recovery during the treatment phase. However, after washout, younger men were more likely to achieve recovery.
This aligns with broader literature showing that younger age is a strong predictor of postoperative erectile recovery. The biologic plausibility is straightforward: neural plasticity, vascular health, and smooth muscle integrity decline with age.
For clinicians, this underscores the importance of individualized counseling. Younger men may benefit most from aggressive early rehabilitation strategies, including daily tadalafil.
Practical Implications for Penile Rehabilitation Protocols
The findings of this study have meaningful implications for postoperative management.
Men undergoing bilateral nerve-sparing radical prostatectomy should be counseled preoperatively about:
- Expected timelines of erectile recovery
- The difference between assisted and unassisted erections
- The potential role of daily PDE5 inhibitor therapy
A structured rehabilitation plan may include:
- Early initiation of daily tadalafil (5 mg) within weeks after surgery
- Monitoring of IIEF-EF scores
- Gradual reintroduction of sexual activity
- Consideration of adjunctive therapies (vacuum erection devices, intracavernosal therapy if needed)
Importantly, PRN tadalafil alone may not provide the same rehabilitative effect as daily dosing in the early postoperative phase.
One might say, with measured irony, that penile rehabilitation resembles orthopedic rehabilitation more than it resembles episodic symptom treatment. Continuous therapy appears superior to intermittent effort.
Limitations and Clinical Context
No study is without limitations.
The nine-month double-blind period was insufficient for full spontaneous recovery in many patients. Median time to recovery could not be estimated because fewer than 50% of patients achieved full recovery during treatment.
Additionally, the washout period interrupted therapy, making long-term time-to-event analysis complex.
Finally, the study population consisted of relatively low-risk men (normal preoperative erectile function, organ-confined cancer, high-quality nerve-sparing surgery). Results may differ in older patients or those with comorbidities.
Nevertheless, the methodology was rigorous, the sample size robust, and the conclusions clinically relevant.
The Broader Perspective: Rehabilitation Versus Rescue
The modern approach to erectile dysfunction after prostatectomy must shift from reactive to proactive.
Waiting for spontaneous recovery is no longer the preferred strategy. Evidence increasingly supports early intervention to preserve tissue health and accelerate functional return.
Tadalafil, particularly in a once-daily 5 mg regimen, appears to shorten time to erectile recovery when initiated early after bilateral nerve-sparing surgery.
While it does not guarantee full recovery, it improves the probability of earlier improvement and clinically meaningful gains.
In a condition where recovery may otherwise take 18–24 months, a three-to-four-month acceleration is not trivial.
For many couples, it may represent the difference between despair and hope.
FAQ
1. Does daily tadalafil permanently restore erectile function after prostatectomy?
Daily tadalafil accelerates time to erectile recovery during treatment. However, evidence for permanent enhancement of unassisted recovery after drug discontinuation remains less definitive. It appears to speed recovery rather than fundamentally alter the eventual recovery ceiling.
2. Is once-daily tadalafil better than taking it only when needed?
Yes, in the early postoperative period after bilateral nerve-sparing radical prostatectomy, once-daily tadalafil significantly shortened time to recovery compared to placebo, while PRN dosing did not show the same statistically significant effect.
3. When should tadalafil be started after prostatectomy?
Evidence suggests that early initiation—soon after surgery once medically appropriate—may provide the greatest rehabilitative benefit. Delayed initiation may reduce potential impact on tissue preservation and recovery acceleration.
