

Introduction: When Common Conditions Become Systemic Burdens
Erectile dysfunction (ED) and benign prostatic hyperplasia-associated lower urinary tract symptoms (BPH-LUTS) are among the most prevalent chronic conditions affecting aging men. Individually, each condition carries a measurable burden. Together, they create a clinical and economic challenge that extends far beyond the urology clinic.
Modern medicine often evaluates treatments based on efficacy and safety. However, an equally important question is frequently overlooked: how do these therapies influence the broader healthcare system? Do they reduce hospital visits, minimize diagnostic testing, and improve long-term adherence?
The retrospective database study addresses precisely this question. It shifts the focus from isolated clinical outcomes to real-world healthcare resource utilization (HCRU), offering a rare and valuable perspective. The findings are both clinically meaningful and economically relevant: patients treated with tadalafil demonstrate lower healthcare utilization and better treatment persistence compared to those not receiving PDE5 inhibitors.
In other words, the right drug may not only treat symptoms—it may quietly reduce the entire burden of care.
The Interconnected Pathophysiology of ED and BPH-LUTS
At first glance, ED and BPH-LUTS may appear as separate entities—one affecting sexual function, the other urinary flow. In reality, they are deeply interconnected.
Both conditions share common risk factors, including aging, metabolic disease, hypertension, and endothelial dysfunction. The study highlights that men with ED are significantly more likely to develop BPH-LUTS, and vice versa . This relationship persists even after controlling for confounding variables, suggesting a shared biological pathway.
Central to this connection is the nitric oxide (NO) signaling cascade. Reduced NO availability leads to impaired smooth muscle relaxation in both penile and prostatic tissues. The result is compromised blood flow, increased muscle tone, and functional obstruction.
Clinically, this overlap manifests as a dual symptom burden. Patients do not present with isolated complaints—they arrive with a constellation of urinary and sexual dysfunctions that demand a unified therapeutic strategy.
Ignoring this relationship is no longer an option.
Real-World Evidence: Moving Beyond Controlled Trials
Randomized controlled trials remain the gold standard of clinical research. However, they often fail to capture the complexity of everyday medical practice.
The study analyzed data from the IQVIA US PharMetrics Plus database, encompassing over 60,000 patients. This real-world evidence approach provides insights into actual prescribing patterns, patient behavior, and healthcare utilization over time.
Unlike controlled trials, this dataset reflects the variability of real patients—those with comorbidities, inconsistent adherence, and diverse healthcare access. It includes men aged 45 and older with both ED and BPH-LUTS, followed over a 12-month period.
This design allows for a comprehensive evaluation of how tadalafil performs outside the controlled environment of clinical trials.
And the answer is clear: it performs well—consistently and across multiple dimensions.
Healthcare Resource Utilization: A Hidden Metric of Success
Healthcare resource utilization is an indirect but powerful measure of treatment effectiveness. It reflects not only symptom control but also disease stability and patient satisfaction.
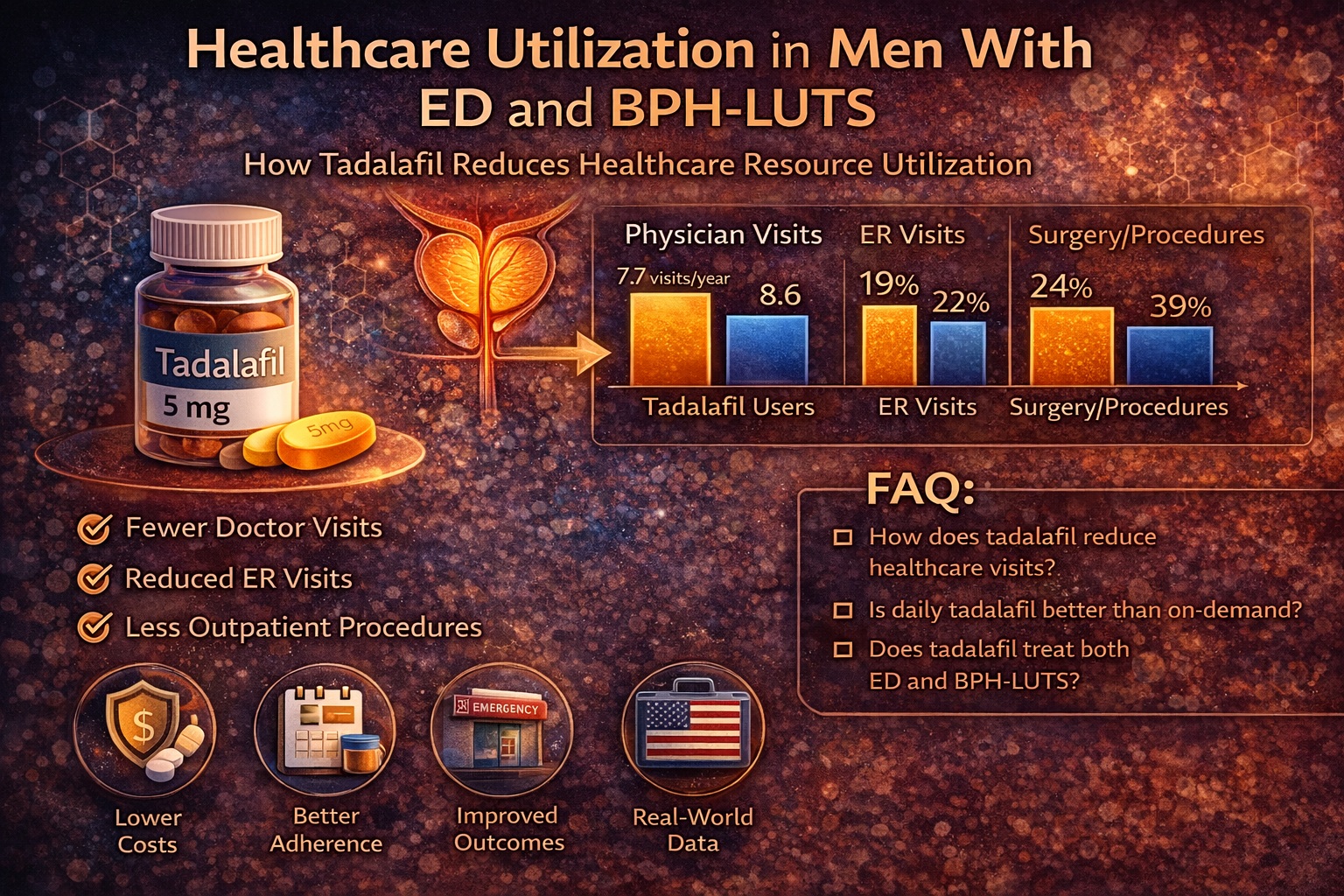
The study demonstrates that patients treated with tadalafil required fewer healthcare services across multiple categories:
- Fewer physician office visits
- Reduced laboratory and radiology testing
- Lower rates of outpatient surgical procedures
- Decreased emergency room visits and hospitalizations
For example, the proportion of patients with at least one emergency room visit was significantly lower in the tadalafil group (18.6% vs 21.7%). Similarly, outpatient surgical visits were reduced (63.0% vs 68.8%).
These differences may appear modest at the individual level. However, when extrapolated across populations, they represent substantial reductions in healthcare burden.
In practical terms, fewer visits mean less disruption for patients—and lower costs for healthcare systems.
Disease-Specific Utilization: Precision Benefits of Targeted Therapy
When examining disease-specific outcomes, the advantages of tadalafil become even more pronounced.
Patients treated with tadalafil showed significantly lower utilization of services directly related to ED and BPH-LUTS. This includes fewer:
- Specialist consultations
- Diagnostic procedures
- Surgical interventions
- Ancillary services
Notably, only 55.1% of tadalafil-treated patients required disease-specific physician visits, compared to 91.4% in the non-PDE5i group. Laboratory testing and outpatient procedures followed a similar pattern.
This suggests that tadalafil does more than alleviate symptoms—it stabilizes the disease process.
From a clinical perspective, this is the hallmark of effective therapy: fewer interventions are needed because fewer problems arise.
Adherence and Persistence: The Achilles’ Heel of Chronic Therapy
Even the most effective drug fails if patients do not take it. Adherence and persistence are therefore critical determinants of real-world success.
The study reveals a striking difference between dosing strategies. Patients receiving once-daily tadalafil (2.5 or 5 mg) demonstrated significantly higher adherence and persistence compared to those using higher, as-needed doses.
Mean persistence reached nearly 180 days for daily dosing, compared to just over 60 days for on-demand use. Similarly, adherence (measured as proportion of days covered) was more than double in the daily dosing group .
This finding is not surprising. Daily regimens integrate more naturally into routine, reducing the cognitive burden of treatment.
There is also a psychological component. Daily therapy reinforces the perception of continuous care, while on-demand use may be associated with episodic or inconsistent engagement.
In short, simplicity improves compliance—and compliance improves outcomes.
Clinical Profiles: Who Benefits Most from Tadalafil?
The study population reflects a typical cohort of men with ED and BPH-LUTS: middle-aged, with a high prevalence of comorbidities such as hypertension, dyslipidemia, and diabetes.
Interestingly, a large proportion of tadalafil patients were already receiving α1-blockers, particularly tamsulosin, prior to initiating therapy . This suggests that tadalafil is often introduced as part of combination or sequential therapy.
Patients in the tadalafil group also demonstrated slightly lower rates of emergency visits and certain comorbid conditions at baseline. While these differences are modest, they may reflect physician selection bias.
Nevertheless, the overall consistency of outcomes across diverse patient profiles supports the generalizability of the findings.
Tadalafil appears to be effective not only in ideal candidates, but in the heterogeneous population encountered in everyday practice.
Economic and System-Level Implications
From a health economics perspective, the implications of reduced healthcare utilization are profound.
Lower rates of physician visits, diagnostic testing, and surgical procedures translate directly into cost savings. While the study does not provide direct cost analyses, the reduction in resource utilization strongly suggests economic benefit.
Moreover, improved adherence reduces the need for treatment escalation and minimizes complications.
In an era of value-based care, therapies that deliver both clinical and economic benefits are highly desirable.
Tadalafil, in this context, is more than a symptom-relief agent—it is a system-level intervention.
Limitations: Interpreting Real-World Data with Caution
No study is without limitations, and real-world evidence carries inherent challenges.
The use of claims data introduces the possibility of coding errors and incomplete clinical information. Additionally, observational studies cannot establish causality—only associations.
The study also excludes certain populations, such as older patients not covered by specific insurance plans, which may limit generalizability.
Finally, adherence metrics based on prescription fills do not guarantee actual medication use.
Despite these limitations, the large sample size and consistency of findings provide strong support for the conclusions.
Conclusion: Redefining Value in Urological Therapy
The management of ED and BPH-LUTS is evolving. The focus is shifting from isolated symptom control to comprehensive care that addresses clinical outcomes, patient behavior, and healthcare utilization.
This study demonstrates that tadalafil plays a central role in this transformation. It reduces healthcare resource utilization, improves adherence, and provides effective symptom relief.
Perhaps most importantly, it highlights a broader truth: the value of a therapy extends beyond its pharmacology. It lies in its ability to simplify care, improve patient experience, and reduce the burden on healthcare systems.
In that sense, tadalafil is not just a drug—it is a strategy.
FAQ: Practical Questions About Tadalafil and Healthcare Utilization
1. Does tadalafil reduce the need for doctor visits?
Yes. Patients treated with tadalafil had fewer physician visits and diagnostic procedures.
2. Why is daily tadalafil more effective than on-demand use?
Daily dosing improves adherence and provides continuous symptom control.
3. Does tadalafil help both ED and urinary symptoms?
Yes. It targets shared pathways, improving both conditions simultaneously.
4. Is tadalafil cost-effective?
Indirectly, yes. Reduced healthcare utilization suggests lower overall costs.
5. Who should consider tadalafil therapy?
Men with both ED and BPH-LUTS, especially those seeking a unified and convenient treatment approach.
