

Introduction: A Rare Emergency with a Preventable Trigger
Medicine often teaches through patterns—common symptoms, familiar mechanisms, predictable outcomes. Yet occasionally, a single case disrupts this order, forcing clinicians to reconsider what they thought they understood.
Priapism is one such condition. Rare, dramatic, and urgent, it is usually discussed in textbooks as a complication of hematologic disorders or isolated drug effects. But the case presented in introduces a more unsettling scenario: a severe, refractory ischemic priapism triggered not by one drug, but by the interaction between two—chlorpromazine and tadalafil.
This is not merely a case report. It is a cautionary tale about pharmacological synergy, self-medication, and the consequences of overlooking drug interactions. The outcome—penile prosthesis implantation—marks the failure of conventional management and the irreversible nature of delayed intervention.
In this article, we examine this case through a clinical lens, expanding its implications into a broader discussion of physiology, pharmacology, and patient safety.
Understanding Priapism: More Than a Prolonged Erection
Priapism is defined as a persistent penile erection lasting more than four hours, unrelated to sexual stimulation and unrelieved by ejaculation. While the definition is simple, the condition itself is anything but.
Clinically, priapism is categorized into three types: ischemic (low-flow), non-ischemic (high-flow), and stuttering (recurrent). Among these, ischemic priapism is the most common—and the most dangerous.
In ischemic priapism, venous outflow is obstructed, leading to blood stasis within the corpora cavernosa. Over time, this stagnant blood becomes hypoxic and acidotic, initiating a cascade of tissue injury. As noted on page 2, prolonged ischemia results in necrosis, fibrosis, and ultimately irreversible erectile dysfunction .
Time is critical. Beyond 24–36 hours, the likelihood of permanent damage increases dramatically. At 72 hours—as in this case—the prognosis is poor, regardless of intervention.
Priapism, therefore, is not merely an inconvenience. It is a race against irreversible tissue loss.
The Case: A Timeline of Escalation
The patient—a 56-year-old man—presented with a painful erection persisting for 72 hours. His medical history was largely unremarkable, but his medication history told a different story.
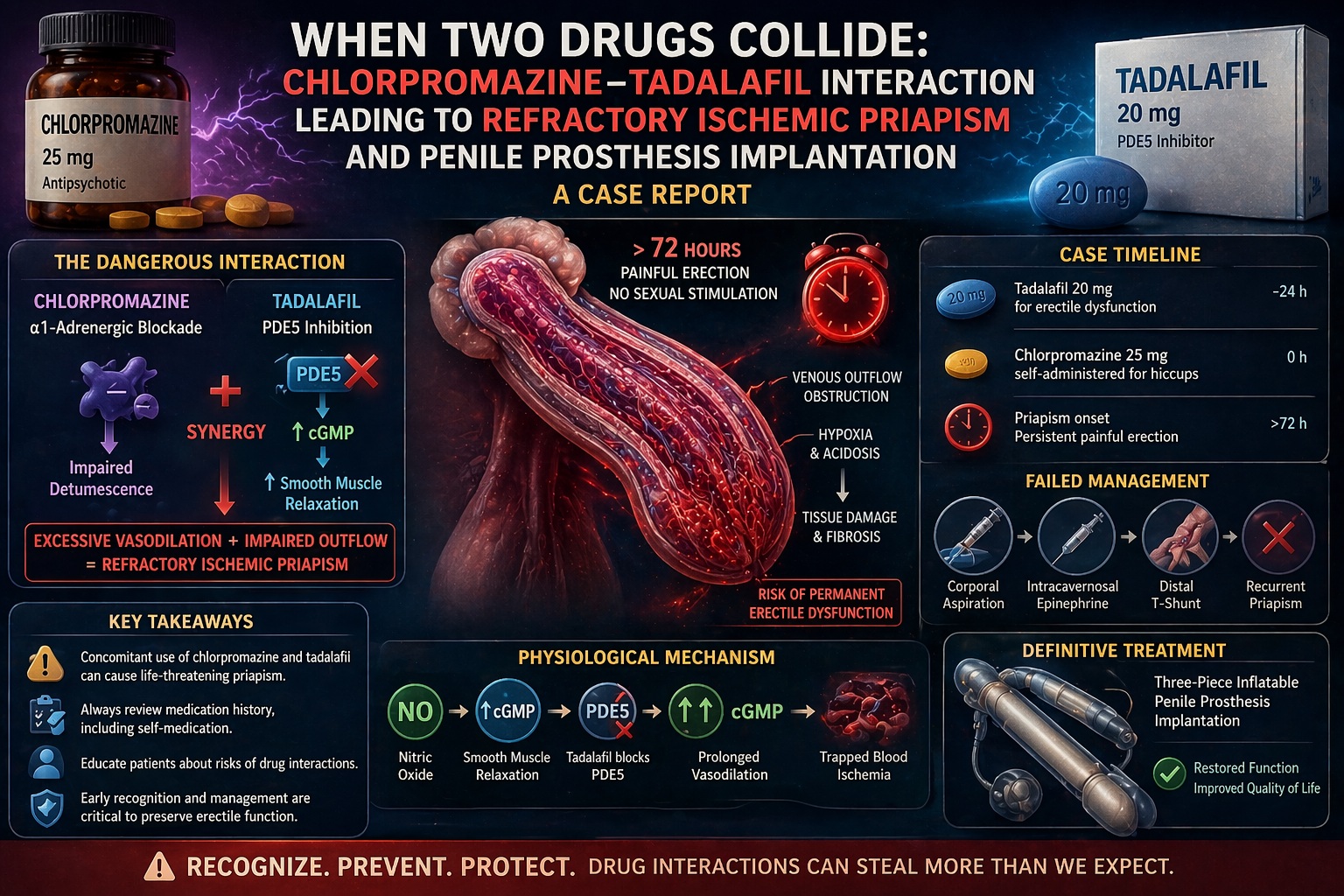
Approximately 24 hours before symptom onset, he had taken tadalafil 20 mg for erectile dysfunction. Later, he self-administered chlorpromazine 25 mg for persistent hiccups—an off-label but not uncommon use.
Crucially, this was not his first encounter with chlorpromazine-induced priapism. Ten years earlier, he had experienced a transient episode following the same drug, though it resolved spontaneously .
This time, however, the presence of tadalafil changed everything.
Despite standard treatment—including aspiration, intracavernosal epinephrine, and a distal T-shunt procedure—the priapism persisted. Recurrence occurred even after initial detumescence, indicating profound disruption of normal erectile physiology.
Ultimately, the only viable option was implantation of a three-piece penile prosthesis—a definitive but irreversible solution.
Pharmacological Synergy: When Mechanisms Overlap
The severity of this case lies not in either drug alone, but in their interaction.
Chlorpromazine, a first-generation antipsychotic, exerts its effect through alpha-1 adrenergic receptor blockade. This mechanism interferes with detumescence—the physiological process by which an erection subsides.
Tadalafil, on the other hand, enhances nitric oxide–mediated vasodilation by inhibiting phosphodiesterase type 5 (PDE5). This increases cGMP levels, promoting sustained smooth muscle relaxation and increased blood flow.
Individually, these mechanisms are well understood. Together, they create a perfect storm.
As described on page 4, the combination leads to synergistic impairment of erectile regulation: reduced outflow (via alpha blockade) and increased inflow (via PDE5 inhibition) .
To complicate matters further, chlorpromazine may inhibit CYP3A4—the enzyme responsible for metabolizing tadalafil. This prolongs tadalafil’s activity, extending its effects well beyond the expected window.
The result is not simply additive—it is exponential.
Pharmacokinetics: The Role of Time and Accumulation
Timing is everything in pharmacology.
Tadalafil has a half-life of approximately 17.5 hours, with clinical effects lasting up to 36 hours. Chlorpromazine, meanwhile, has a half-life of around 30 hours.
In this case, the patient took chlorpromazine while tadalafil was still pharmacologically active. A second dose of chlorpromazine further compounded the effect, leading to drug accumulation.
This temporal overlap is critical. It transformed a manageable risk into a refractory condition.
As noted on page 4, the dose–response relationship was evident: a single dose of chlorpromazine previously caused transient priapism, while repeated dosing in the presence of tadalafil resulted in a persistent and severe episode .
This illustrates a fundamental principle: drug interactions are not only about mechanism, but also about timing.
Diagnosis: Confirming Ischemia and Excluding Alternatives
The diagnostic process in this case was thorough and methodical.
Corporal blood gas analysis revealed a pH of 6.9, pO₂ of 28 mmHg, and pCO₂ of 60 mmHg—findings consistent with ischemic priapism. These values reflect severe hypoxia and acidosis within the penile tissue.
Comprehensive toxicological screening ruled out recreational drugs and other potential causes. Hematologic conditions such as sickle cell disease were also excluded.
This systematic approach strengthens the causal link between the drug interaction and the clinical outcome.
Using the Naranjo Adverse Drug Reaction Probability Scale, the case achieved a score of 9—indicating a definite drug-related event .
In clinical terms, this is as close to certainty as one can reasonably achieve.
Management: When Standard Protocols Fail
The management of ischemic priapism follows a well-established algorithm.
First-line treatment involves aspiration of corporal blood and irrigation, followed by intracavernosal injection of sympathomimetic agents. These interventions aim to restore normal blood flow and relieve pressure.
When these measures fail, surgical options are considered. In this case, a distal T-shunt was performed, achieving temporary success.
However, recurrence occurred within hours—an indication of severe underlying pathology.
At this stage, further conservative measures were unlikely to succeed. As recommended on page 4, early penile prosthesis implantation is indicated in cases of prolonged, refractory priapism .
The decision is not taken lightly. It represents the end of one function and the beginning of another.
Penile Prosthesis: A Definitive but Final Solution
Penile prosthesis implantation is both a therapeutic and restorative procedure.
In this case, a three-piece inflatable prosthesis was implanted. The procedure achieved immediate detumescence and prevented further tissue damage.
At three-month follow-up, the patient reported satisfactory functional outcomes, including the ability to engage in sexual activity and satisfaction with cosmetic results .
While this outcome is encouraging, it does not negate the loss of natural erectile function.
The prosthesis is a solution—but also a reminder of what was lost.
Clinical Implications: Prevention Over Intervention
This case offers several important lessons for clinical practice.
First, medication history must be comprehensive and precise. Patients may not volunteer information about drugs such as tadalafil, particularly when obtained without prescription.
Second, clinicians must recognize high-risk combinations. The interaction between alpha-blockers and PDE5 inhibitors is not theoretical—it is clinically significant.
Third, patient education is essential. As emphasized on page 5, patients should be warned about the risks of combining these medications and advised on safer alternatives for conditions such as hiccups .
Finally, pharmacovigilance matters. Reporting such cases contributes to a broader understanding of drug safety and informs future practice.
In many cases, prevention is not just better than cure—it is the only cure.
Limitations and Broader Context
As a single case report, this study cannot establish generalizable conclusions. However, its strength lies in its clarity.
The temporal relationship, prior history, exclusion of alternatives, and biological plausibility create a compelling narrative.
The absence of serum drug levels is a limitation, as is the lack of long-term follow-up. Genetic factors influencing drug metabolism were not assessed.
Nevertheless, the case provides valuable insight into a rare but serious interaction.
In medicine, even one case can change practice—if it is understood correctly.
Conclusion: A Lesson in Pharmacological Vigilance
The interaction between chlorpromazine and tadalafil in this case represents more than an unfortunate coincidence. It is a predictable outcome of overlapping pharmacological mechanisms.
The tragedy lies not in the rarity of the event, but in its preventability.
For clinicians, the message is clear: understand your drugs, know their interactions, and never underestimate the importance of timing.
Because in medicine, as in life, it is often not what we use—but how and when we use it—that determines the outcome.
FAQ: Key Questions About Priapism and Drug Interactions
1. What causes ischemic priapism?
It results from impaired venous outflow, leading to blood stasis, hypoxia, and tissue damage.
2. Can tadalafil alone cause priapism?
Rarely. The risk increases significantly when combined with other drugs affecting erectile physiology.
3. Why is chlorpromazine risky?
It blocks alpha-1 receptors, preventing detumescence and increasing the risk of prolonged erections.
4. When is surgery necessary?
If priapism persists beyond 24–36 hours or fails to respond to standard treatment, surgical intervention may be required.
5. Can this condition be prevented?
Yes. Avoiding high-risk drug combinations and ensuring proper medical guidance significantly reduces risk.
