

Introduction: When the Patient Becomes the Outcome
Erectile dysfunction (ED) is one of the few medical conditions where success cannot be measured by laboratory values, imaging, or biomarkers. It is, fundamentally, a subjective experience. Either the patient is satisfied—or he is not. And in this rare domain of medicine, that distinction defines everything.
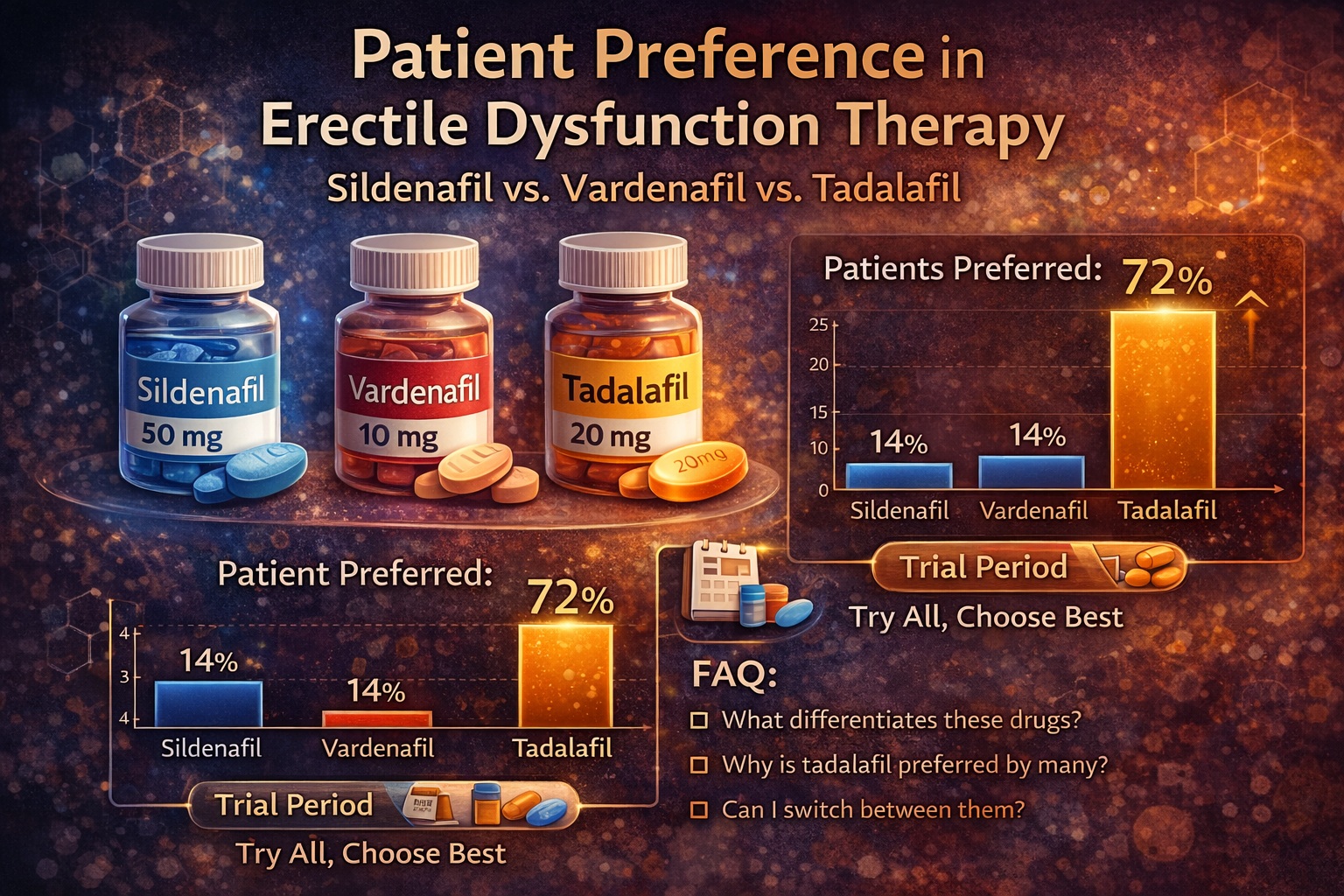
The emergence of oral phosphodiesterase type 5 (PDE5) inhibitors transformed ED management. Sildenafil, vardenafil, and tadalafil offered safe, effective, and non-invasive solutions. Yet with multiple options came a new question: not which drug works, but which one is preferred.
The article under review addresses this exact dilemma. Its conclusion is both pragmatic and slightly inconvenient for those seeking simple answers: no single PDE5 inhibitor is universally superior. Instead, treatment success depends on aligning pharmacology with patient expectations, lifestyle, and relational dynamics .
In other words, the best drug is not chosen by the physician—it is selected by the patient.
Erectile Dysfunction: A Clinical Condition with Psychological Weight
Erectile dysfunction affects up to 52% of men between the ages of 40 and 70, making it one of the most prevalent male health conditions . Yet prevalence statistics only hint at the true burden.
ED is not merely a physical impairment. It carries significant psychological consequences, including reduced self-esteem, anxiety, and even depression. The condition often extends beyond the individual, affecting partner satisfaction and relationship stability.
The etiology of ED is complex. It may arise from vascular disease, neurological impairment, hormonal imbalance, or psychological factors. In most cases, these elements coexist, creating a multifactorial condition that resists simplistic solutions.
This complexity has important implications. It means that treatment must address not only physiology, but also perception, expectation, and emotional context. A drug that restores erection but fails to restore confidence is, clinically speaking, incomplete.
Mechanism of Action: Shared Pathways, Different Experiences
All three PDE5 inhibitors—sildenafil, vardenafil, and tadalafil—share a common mechanism. They inhibit the enzyme phosphodiesterase type 5, preventing the breakdown of cyclic guanosine monophosphate (cGMP). This enhances nitric oxide–mediated vasodilation, allowing increased blood flow to the corpus cavernosum and facilitating erection.
From a biochemical perspective, the drugs are remarkably similar. Their differences lie not in what they do, but in how long and how predictably they do it.
Sildenafil and vardenafil have relatively short half-lives of approximately 4–5 hours. Tadalafil, by contrast, has a half-life of 17.5 hours, allowing a therapeutic window of up to 36 hours .
This distinction is more than pharmacokinetic trivia. It shapes the patient experience. Short-acting drugs require planning; long-acting drugs allow spontaneity. And in matters of intimacy, timing is not a minor detail—it is the central narrative.
Pharmacokinetics and Lifestyle: Where Tadalafil Stands Apart
Among the three PDE5 inhibitors, tadalafil occupies a unique position. Its prolonged duration of action allows for a more flexible approach to sexual activity, reducing the need for precise timing.
Food interactions further differentiate these agents. High-fat meals can delay the absorption of sildenafil and vardenafil, whereas tadalafil remains unaffected . For patients, this translates into fewer restrictions and a more natural integration into daily life.
These pharmacokinetic advantages are not merely theoretical. They directly influence patient preference. Studies consistently show that many men value spontaneity and freedom from scheduling constraints—factors that tadalafil uniquely supports.
However, it would be an oversimplification to declare tadalafil the universal winner. While its duration is appealing, some patients prefer the predictability and rapid onset of shorter-acting agents.
In medicine, as in life, convenience is subjective.
Efficacy and Safety: A Level Playing Field
All three PDE5 inhibitors have demonstrated strong efficacy across a broad range of patients, including those with diabetes, cardiovascular disease, and other comorbidities. Response rates are high, and non-responders to one agent may respond to another .
Side effect profiles are also similar. Common adverse events include headache, flushing, dyspepsia, and nasal congestion. These effects are generally mild and lead to discontinuation in only 1–2% of cases.
Each drug has its own subtle signature. Sildenafil is associated with visual disturbances, likely due to PDE6 inhibition. Tadalafil, on the other hand, may cause back pain—a side effect that is both distinctive and, for most patients, tolerable.
From a safety perspective, none of the three drugs holds a decisive advantage. This parity reinforces the importance of patient preference as the primary differentiating factor.
Patient Preference: The Central Determinant of Success
Unlike most medical treatments, ED therapy is judged almost entirely by patient-reported outcomes. There is no objective test for satisfaction. The patient’s perception is the endpoint.
Several studies have attempted to quantify preference among PDE5 inhibitors. Many have shown a tendency toward tadalafil, often attributed to its longer duration of action. For example, in one crossover study, 73% of patients preferred tadalafil over sildenafil .
Other studies report even higher preference rates, with up to 82–90% of patients favoring tadalafil in certain contexts. The reasons cited include improved spontaneity, reduced performance anxiety, and enhanced sexual confidence.
However, these findings are not universal. Independent studies have shown no significant difference in preference among the three drugs. Some patients prefer sildenafil or vardenafil, particularly those who value rapid onset or have experience with these agents.
The variability underscores a key principle: preference is not determined by pharmacology alone. It is shaped by individual values, expectations, and experiences.
Bias in Preference Studies: Why the Data Are Inconclusive
Interpreting preference studies is not straightforward. Many are subject to methodological limitations that introduce bias.
Common issues include:
- Lack of randomization or blinding
- Unequal treatment durations
- Carryover effects between study phases
- Selection bias in patient populations
For example, patients previously satisfied with sildenafil may be more likely to remain loyal to it, while those seeking alternatives may favor newer agents. Industry-sponsored studies may also influence outcomes, consciously or otherwise.
As highlighted in the review, no single study provides definitive evidence of superiority. Instead, the collective data suggest equivalence in efficacy, with differences emerging primarily in user experience .
This ambiguity is not a failure of research—it is a reflection of human variability.
Factors Influencing Choice: Beyond the Prescription
Patient preference is influenced by a complex interplay of factors, many of which extend beyond the drug itself.
These include:
- Lifestyle and relationship dynamics
- Cultural attitudes toward sexuality
- Financial considerations
- Comorbid conditions and concurrent medications
- Physician experience and recommendations
For some patients, the ability to plan intercourse precisely is reassuring. For others, it is a source of anxiety. Some value spontaneity; others prefer predictability.
Interestingly, a subset of patients may even prefer a combination approach—using both short- and long-acting agents depending on circumstances. This flexibility reflects the nuanced nature of sexual behavior.
In this context, the role of the clinician is not to dictate choice, but to facilitate it.
Clinical Strategy: Letting the Patient Decide
Given the lack of clear superiority among PDE5 inhibitors, the most effective clinical strategy is surprisingly simple: allow the patient to try all three options.
This approach is supported by the literature and aligns with patient-centered care. By experiencing each drug firsthand, patients can make informed decisions based on their own preferences and outcomes.
This strategy has several advantages. It increases the likelihood of treatment success, improves adherence, and fosters a sense of autonomy.
It also acknowledges a fundamental truth: medicine is not practiced in a vacuum. It exists within the context of individual lives, relationships, and expectations.
Conclusion: Preference as a Clinical Endpoint
The comparison of sildenafil, vardenafil, and tadalafil reveals an important insight: in erectile dysfunction therapy, the concept of “best” is inherently subjective.
All three drugs are effective, safe, and well tolerated. Their differences lie in pharmacokinetics, user experience, and alignment with patient lifestyle.
Tadalafil, with its extended duration, offers a unique advantage in promoting spontaneity. For many patients, this is a decisive factor. For others, it is less important.
Ultimately, the success of ED therapy depends not on the drug itself, but on how well it fits the patient’s life. And that is a decision only the patient can make.
FAQ: Key Questions About PDE5 Inhibitor Choice
1. Is one PDE5 inhibitor better than the others?
No. All three are effective and safe; differences are mainly in duration and user experience.
2. Why do many patients prefer tadalafil?
Because of its long duration of action, which allows greater spontaneity.
3. Can patients switch between PDE5 inhibitors?
Yes. Patients who do not respond to one may respond to another.
4. Are side effects different between drugs?
They are similar overall, with minor differences such as back pain (tadalafil) and visual effects (sildenafil).
5. What is the best way to choose a treatment?
The most effective approach is to try different options and select the one that best suits the patient and his partner.
