

Introduction: A Trusted Drug with an Unexpected Face
Tadalafil is widely regarded as a predictable and well-tolerated medication. As a phosphodiesterase-5 (PDE-5) inhibitor, it has earned its place in modern therapeutics for erectile dysfunction, pulmonary arterial hypertension, and benign prostatic hyperplasia. Its pharmacological profile is stable, its dosing flexible, and its adverse effects—headache, dyspepsia, nasal congestion—generally mild and transient.
Yet even familiar drugs can surprise us.
Cutaneous adverse drug reactions remain one of the most complex and diagnostically challenging domains in clinical medicine. Among these reactions, fixed drug eruption (FDE) is distinctive for its almost theatrical precision: each re-exposure to the offending agent produces lesions in the exact same anatomical locations. While FDE itself is not rare, its generalized bullous variant (GBFDE) is far less common and can closely resemble life-threatening dermatoses such as Stevens–Johnson syndrome (SJS) or toxic epidermal necrolysis (TEN).
The case described in the source article documents what appears to be the first reported instance of generalized bullous fixed drug eruption induced by tadalafil. This article explores the clinical, pathological, immunological, and public health implications of that observation.
Understanding Fixed Drug Eruption: A Reaction That Remembers
Fixed drug eruption is a type IV hypersensitivity reaction mediated primarily by CD8+ T lymphocytes. Unlike many drug eruptions that produce diffuse or unpredictable lesions, FDE is characterized by its recurrence at “fixed” sites. The immune system, once sensitized, responds to the drug by targeting previously affected skin areas with remarkable consistency.
Clinically, classic FDE presents as sharply demarcated, round or oval erythematous patches with a violaceous hue. Over time, these lesions may blister. Upon resolution, they often leave behind residual hyperpigmentation—a visible reminder of the immune system’s memory. The lips, genitalia, trunk, and extremities are common sites, though any mucocutaneous region can be involved.
With each re-exposure, the reaction may intensify. What begins as a solitary patch may evolve into multiple lesions. In rare circumstances, blistering becomes widespread, crossing the threshold into generalized bullous fixed drug eruption.
It is precisely this escalation that transforms a manageable dermatologic reaction into a potentially severe systemic concern.
Generalized Bullous Fixed Drug Eruption: A Dangerous Mimic
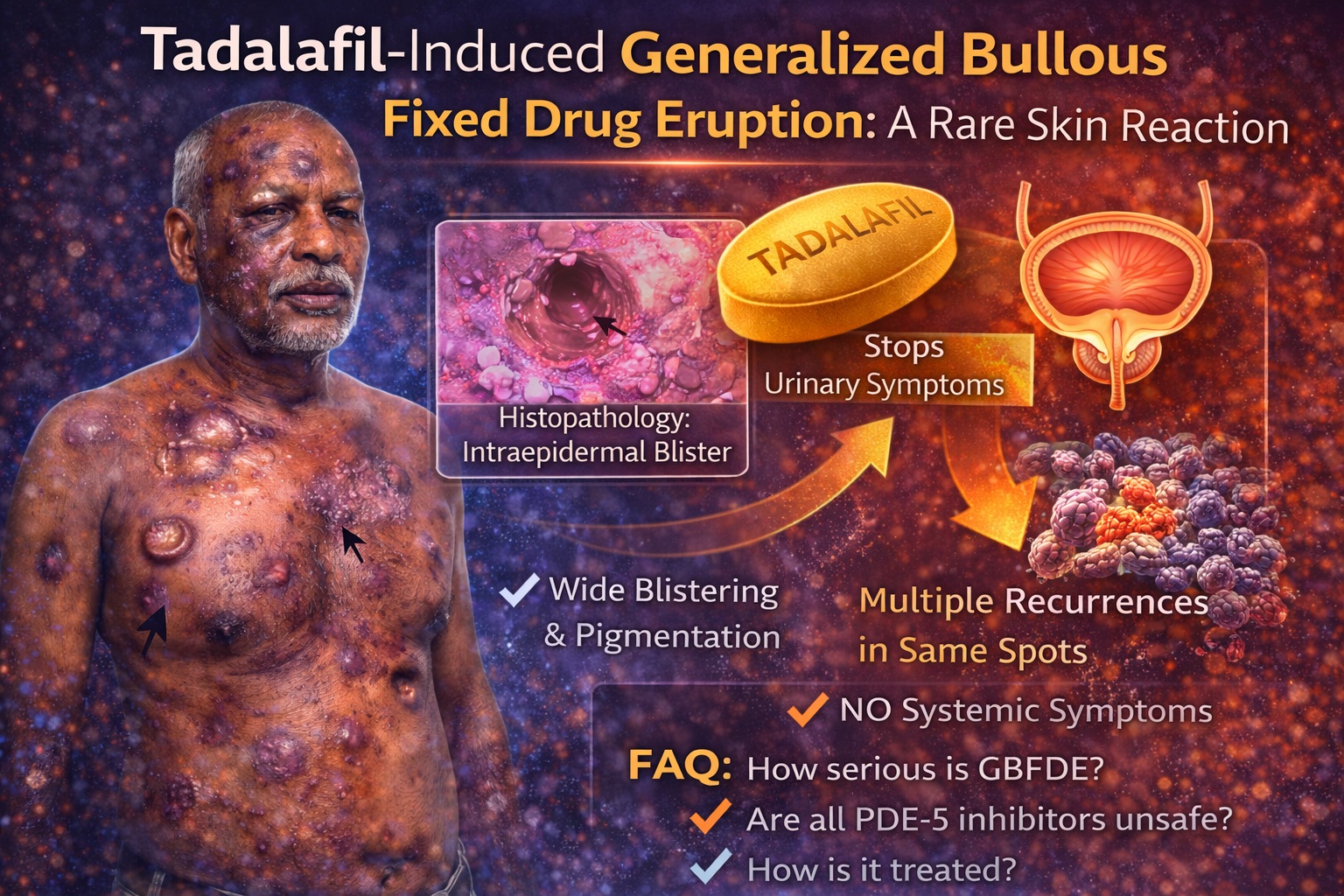
Generalized bullous fixed drug eruption is defined by extensive blistering superimposed on typical FDE lesions. Diagnostic criteria include involvement of at least three of six anatomical regions—head and neck, anterior trunk, posterior trunk, upper limbs, lower limbs, and genitalia—or involvement of more than 10% of total body surface area.
The clinical challenge lies in differentiation. GBFDE can resemble SJS or TEN, conditions associated with high morbidity and mortality. However, important distinctions exist. In GBFDE, lesions recur in identical locations upon re-exposure, and systemic symptoms such as fever and malaise may be minimal or absent. Histopathology reveals intraepidermal blistering with basal layer hydropic degeneration and inflammatory infiltrates, often containing eosinophils.
In the reported case , blistering involved multiple anatomical regions including trunk, extremities, lips, and genitalia—meeting criteria for generalized involvement. Importantly, the patient lacked systemic symptoms, and laboratory investigations were unremarkable, helping to differentiate GBFDE from more catastrophic drug reactions.
Clinicians must recognize that not all widespread bullous eruptions herald systemic collapse—but careful evaluation is mandatory.
The Case in Focus: Clinical Evolution of Tadalafil-Induced GBFDE
The patient was a 46-year-old man presenting with pruritic, mildly painful erythematous patches and vesiculobullous lesions of three days’ duration. Notably, he described two previous similar episodes over the preceding five months, each resolving spontaneously without medical attention.
This history is a diagnostic clue of immense value. Recurrent lesions at identical sites strongly suggest fixed drug eruption. The patient initially denied medication use, a common scenario when the drug involved carries social stigma. Eventually, he disclosed taking an over-the-counter tablet for recreational purposes—later identified as tadalafil 5 mg.
On examination, hyperpigmented patches with violaceous hue were symmetrically distributed across trunk, extremities, lips, and genitalia. Blisters ranging from small vesicles to large bullae were evident across multiple regions. Histopathological examination confirmed intraepidermal bullae, basal layer degeneration, and lymphoeosinophilic infiltrates—classic features of FDE.
Application of the Naranjo adverse drug reaction probability scale yielded a score of 8, indicating a probable causal relationship between tadalafil and the eruption.
The management was straightforward yet decisive: aspiration of large bullae and systemic corticosteroid therapy (prednisolone 40 mg daily). Within 10 days, lesions resolved, leaving mild post-inflammatory hyperpigmentation.
The immune system, however, would not forget.
Pathophysiology: Why Does Fixed Drug Eruption Recur in the Same Spot?
The pathogenesis of FDE reflects localized immune memory. Drug-specific CD8+ memory T cells persist in previously affected skin sites long after clinical resolution. Upon re-exposure to the offending medication, these resident memory cells are rapidly reactivated, triggering keratinocyte apoptosis and inflammatory cascade.
The precise molecular triggers remain under investigation. It is hypothesized that drug metabolites bind to keratinocyte proteins, forming hapten–carrier complexes recognized as foreign. This results in localized cytotoxic response.
In GBFDE, the mechanism is the same but amplified. The reaction is not merely localized but disseminated across multiple sensitized sites. Importantly, the absence of systemic cytokine storm distinguishes GBFDE from SJS/TEN, though overlap can occur.
The immunological paradox is striking: a drug designed to relax vascular smooth muscle can, in rare individuals, provoke aggressive cutaneous immune activation.
Tadalafil: Popular, Accessible, and Increasingly Misused
Tadalafil’s pharmacology is well understood. By inhibiting PDE-5, it increases cyclic guanosine monophosphate (cGMP) levels in vascular smooth muscle, promoting vasodilation and facilitating penile erection. Its longer half-life compared to other PDE-5 inhibitors allows for more flexible dosing.
Beyond erectile dysfunction, tadalafil is approved for pulmonary arterial hypertension and lower urinary tract symptoms associated with benign prostatic hyperplasia. However, its over-the-counter availability in many regions and aggressive marketing have expanded its use beyond medical necessity.
Recreational consumption is rising. Cultural taboos surrounding sexual health often discourage open discussion, leading individuals to self-medicate without professional oversight. When adverse reactions occur, patients may hesitate to disclose usage.
This creates a silent gap in pharmacovigilance.
Cutaneous reactions such as FDE may be underreported precisely because the triggering drug carries social sensitivity. In the case described , initial denial of medication intake delayed identification of the culprit.
In medicine, history remains our most powerful diagnostic tool—provided the patient feels safe enough to share it.
Differential Diagnosis and Clinical Approach
When confronted with generalized blistering eruptions, clinicians must consider a broad differential diagnosis. SJS, TEN, bullous pemphigoid, erythema multiforme major, and disseminated herpes infection must all be excluded.
Key distinguishing features of GBFDE include:
- Recurrence at identical anatomical sites
- Well-demarcated hyperpigmented patches
- Relative absence of systemic symptoms
- Rapid improvement after drug withdrawal
Histopathology supports the diagnosis but must be interpreted in clinical context.
Management begins with immediate cessation of the offending drug. In localized FDE, topical corticosteroids and antihistamines are often sufficient. In generalized or bullous forms, systemic corticosteroids may be required. Most cases resolve without scarring, though residual hyperpigmentation is common.
Equally important is patient education. Avoidance of the culprit drug—and chemically related agents—is imperative. In this case, counseling regarding tadalafil and similar PDE-5 inhibitors was essential.
Clinical Lessons and Public Health Implications
This case underscores several important lessons.
First, even widely prescribed and seemingly benign medications can produce rare but significant adverse effects. Second, recurrent dermatologic patterns should prompt investigation into episodic drug exposure. Third, social stigma may obscure medication history, delaying diagnosis.
From a public health perspective, increasing non-prescription use of PDE-5 inhibitors raises concerns about unmonitored adverse reactions. Clinicians should inquire sensitively about recreational drug use when evaluating unexplained dermatoses.
Reporting rare adverse reactions strengthens pharmacovigilance databases and improves collective clinical awareness. A single case may alter diagnostic thinking for many future patients.
The irony is clear: a medication intended to enhance quality of life may, in rare circumstances, compromise it through severe cutaneous reaction.
Conclusion: Vigilance in the Age of Common Drugs
Tadalafil remains an effective and generally safe medication when used appropriately. However, this case of generalized bullous fixed drug eruption reminds us that no drug is exempt from unpredictability.
Recognition of FDE patterns, early withdrawal of the offending agent, and appropriate corticosteroid therapy can lead to rapid recovery. Failure to identify the trigger, however, risks recurrence with increasing severity.
In dermatology—as in all of medicine—patterns tell stories. When lesions recur in the same location, the immune system is speaking clearly. Our responsibility is to listen carefully.
FAQ
1. How serious is generalized bullous fixed drug eruption?
GBFDE can be serious because it mimics life-threatening conditions like Stevens–Johnson syndrome. However, unlike SJS/TEN, GBFDE often lacks systemic symptoms and improves rapidly after discontinuation of the offending drug. Prompt recognition is crucial.
2. Can tadalafil commonly cause skin reactions?
Cutaneous reactions to tadalafil are rare. A few cases of fixed drug eruption have been reported, but generalized bullous presentations are extremely uncommon. Most patients tolerate tadalafil well.
3. If someone has FDE from tadalafil, can they take other PDE-5 inhibitors?
Caution is advised. Cross-reactivity between PDE-5 inhibitors is not fully understood. Patients who develop FDE from tadalafil should avoid it and consult a physician before using any similar medication.
