

Introduction: When One Symptom Demands More Than One Solution
Lower urinary tract symptoms (LUTS) associated with benign prostatic hyperplasia (BPH) are rarely life-threatening—but they are persistently life-altering. Patients describe not just difficulty urinating, but disrupted sleep, reduced confidence, and a constant awareness of their own physiology. Add erectile dysfunction (ED) to the equation—and it often does—and the clinical picture becomes even more complex.
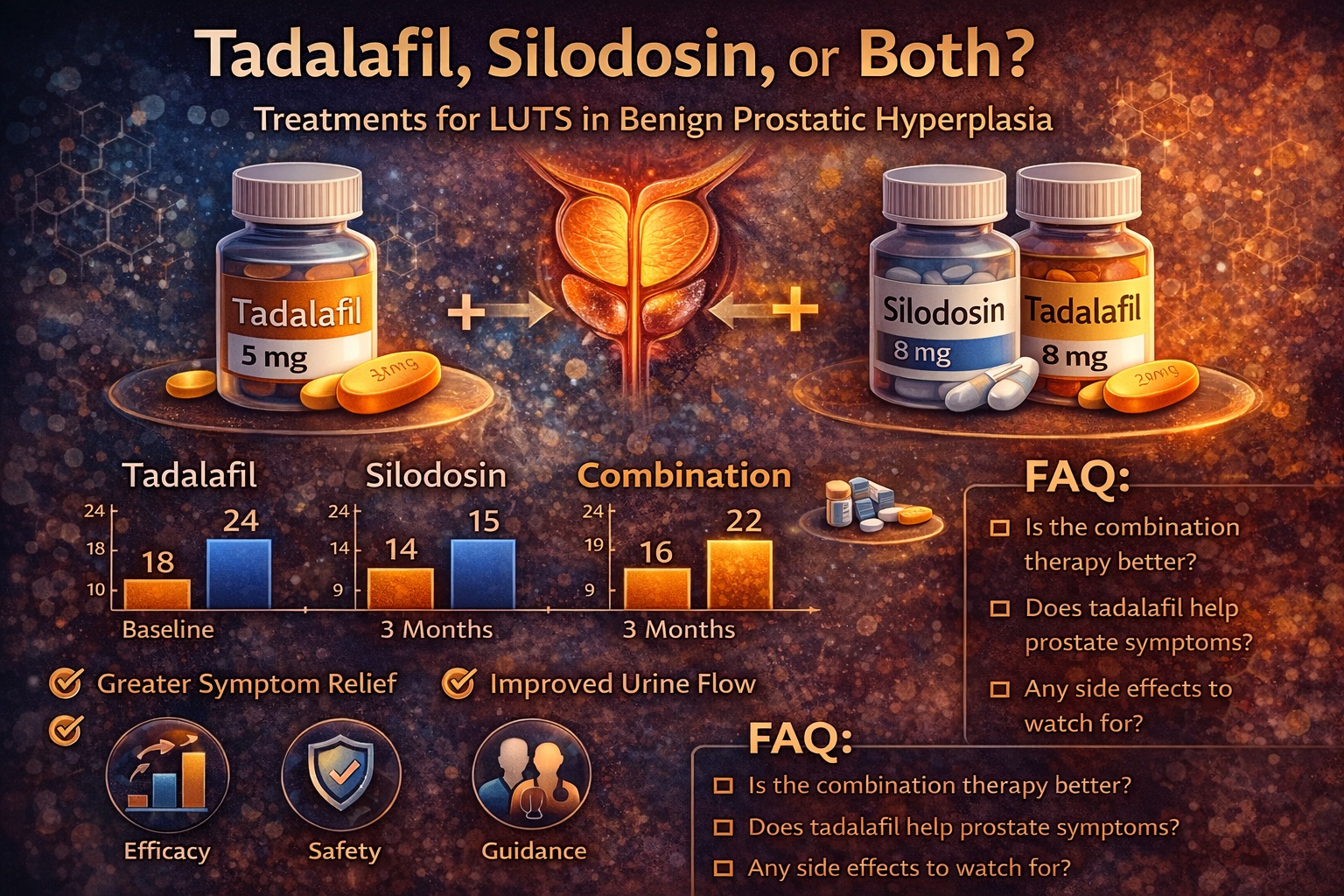
Traditional management has focused on relieving obstruction. Alpha-blockers such as silodosin have long been the cornerstone of therapy. More recently, phosphodiesterase type 5 inhibitors—particularly tadalafil—have expanded the therapeutic landscape by addressing both urinary and sexual symptoms.
The study in focus takes a decisive step forward. Rather than comparing these drugs in isolation, it evaluates them in combination. Its conclusion is straightforward and clinically relevant: both tadalafil and silodosin are effective, but together they are more effective than either alone .
This is not merely an additive effect. It is a paradigm shift—from monotherapy to integrated treatment.
BPH and LUTS: A Multifactorial Disease with Systemic Consequences
Benign prostatic hyperplasia is one of the most common conditions affecting aging men. Its prevalence increases steadily with age, and by the sixth decade of life, a significant proportion of men will experience symptoms.
However, BPH is not simply a matter of prostate size. As the study highlights, only 25–50% of men with anatomical enlargement develop clinical symptoms . This discrepancy underscores the role of additional factors, including smooth muscle tone, bladder function, and neural signaling.
LUTS are typically divided into two categories: storage symptoms (urgency, frequency, nocturia) and voiding symptoms (weak stream, hesitancy, incomplete emptying). Both contribute to reduced quality of life.
Importantly, untreated BPH can lead to complications such as bladder dysfunction, stone formation, hematuria, and even renal impairment. The goal of therapy, therefore, extends beyond symptom relief—it is prevention of disease progression.
Pharmacological Mechanisms: Two Pathways, One Goal
Silodosin and tadalafil represent two distinct pharmacological strategies.
Silodosin is a highly selective α1A-adrenergic receptor antagonist. By relaxing smooth muscle in the prostate and bladder neck, it reduces urethral resistance and improves urinary flow. Its effects are rapid and primarily mechanical.
Tadalafil, on the other hand, operates through the nitric oxide–cGMP pathway. By inhibiting PDE5, it enhances smooth muscle relaxation not only in the corpus cavernosum, but also in the bladder, prostate, and associated vasculature .
This dual mechanism provides a broader physiological effect. It improves blood flow, reduces afferent signaling, and may even exert anti-inflammatory and antifibrotic actions within prostatic tissue.
When combined, these drugs address both dynamic and functional components of LUTS. Silodosin reduces obstruction; tadalafil improves tissue function.
The result is synergy—not redundancy.
Study Design: A Structured Comparison of Three Strategies
The study was conducted as a prospective randomized trial involving more than 300 men with LUTS secondary to BPH. Patients were divided into three groups:
- Tadalafil 5 mg once daily
- Silodosin 8 mg once daily
- Combination therapy with both agents
All patients were followed for three months, with regular assessments of urinary and sexual function.
Baseline characteristics were comparable across groups, including age, prostate volume, symptom severity, and erectile function scores. This balance ensures that observed differences are attributable to treatment rather than patient variability.
Outcome measures included maximum urinary flow rate (Qmax), International Prostate Symptom Score (IPSS), post-void residual urine (PVR), and International Index of Erectile Function (IIEF).
This comprehensive approach captures both objective and subjective dimensions of treatment success.
Urinary Outcomes: Combination Therapy Leads the Field
All three treatment arms demonstrated significant improvement in urinary parameters. This confirms that both tadalafil and silodosin are effective monotherapies.
However, combination therapy consistently outperformed both single agents.
After three months:
- Qmax increased to 15.8 mL/sec in the combination group, compared to 14.4 with tadalafil and 15.2 with silodosin
- IPSS decreased to 15.6 in the combination group, compared to 17.6 and 16.7 in the monotherapy groups
These differences were statistically significant, as shown in the comparative tables on pages 2–4.
Post-void residual urine also improved most in the combination group, indicating more complete bladder emptying.
The pattern is consistent across all parameters: improvement occurs with all treatments, but is greatest when both mechanisms are engaged simultaneously.
Sexual Function: Tadalafil’s Added Value
Erectile function is often overlooked in BPH management, despite its profound impact on quality of life.
In this study, tadalafil—both alone and in combination—significantly improved IIEF scores. Interestingly, silodosin monotherapy also showed improvement, although to a lesser extent .
After treatment:
- IIEF scores increased most in the combination group (21.9)
- Followed by silodosin (21.5) and tadalafil (20.8)
While the differences are modest, they are clinically meaningful. They suggest that combination therapy does not compromise sexual function—in fact, it enhances it.
This is a critical point. Many patients fear that BPH treatment will worsen erectile performance. This study provides reassurance—and perhaps even optimism.
Mechanistic Synergy: Why Combination Works Better
The superiority of combination therapy is not surprising when viewed through a mechanistic lens.
Silodosin reduces urethral resistance by targeting α1 receptors. Tadalafil enhances smooth muscle relaxation and improves blood flow through the NO–cGMP pathway.
Together, these effects address multiple dimensions of LUTS:
- Mechanical obstruction
- Smooth muscle tone
- Vascular perfusion
- Neural signaling
This multidimensional approach mirrors the multifactorial nature of BPH itself.
It also aligns with emerging concepts in urology, where combination therapy is increasingly favored for complex conditions.
Safety and Tolerability: A Manageable Trade-Off
Safety is always a concern when combining pharmacological agents. In this study, adverse events were slightly more frequent in the combination group, but remained mild and manageable.
The most notable side effect was retrograde ejaculation, occurring in:
- 5.9% of patients on silodosin alone
- 9.5% on combination therapy
Other side effects—headache, nasal congestion, dizziness—were infrequent and comparable across groups.
Importantly, no serious complications such as acute urinary retention or prostatitis were reported.
These findings suggest that the benefits of combination therapy outweigh the risks, particularly in appropriately selected patients.
Clinical Implications: Toward Personalized Therapy
The study’s conclusions have direct implications for clinical practice.
Monotherapy with either tadalafil or silodosin is effective and may be sufficient for many patients. However, for those with persistent or severe symptoms, combination therapy offers a superior alternative.
Patient selection becomes key. Factors to consider include:
- Severity of LUTS
- Presence of erectile dysfunction
- Patient preference and tolerance
The study also reinforces the importance of shared decision-making. Treatment should be tailored not only to symptoms, but to patient expectations and lifestyle.
In modern urology, personalization is not optional—it is essential.
Limitations: Context Matters
As with any study, limitations must be acknowledged.
The follow-up period was relatively short (three months), limiting insight into long-term outcomes. The sample size, while adequate, may not capture all variability.
Additionally, the study excluded patients with significant comorbidities, which may limit generalizability.
Despite these limitations, the consistency of findings across multiple parameters supports the validity of the conclusions.
Conclusion: Integration as the Future of BPH Treatment
The management of BPH is evolving. No longer confined to single-drug strategies, it is moving toward integrated approaches that address the full spectrum of symptoms.
This study provides strong evidence that combining tadalafil with silodosin offers superior outcomes in men with LUTS. It improves urinary flow, reduces symptom burden, and enhances erectile function—all with acceptable safety.
In practical terms, it offers clinicians a powerful tool—and patients a more complete solution.
Because in the end, effective treatment is not about choosing one pathway over another. It is about using both.
FAQ: Key Questions About Tadalafil and Silodosin in BPH
1. Is combination therapy better than single-drug treatment?
Yes. It provides greater improvement in urinary symptoms and flow rates.
2. Does tadalafil help with urinary symptoms?
Yes. It improves LUTS through smooth muscle relaxation and enhanced blood flow.
3. Will combination therapy affect sexual function?
No. It may actually improve erectile function.
4. Are side effects more common with combination therapy?
Slightly, but they are generally mild and manageable.
5. Who should consider combination therapy?
Patients with moderate to severe LUTS, especially those with concurrent erectile dysfunction.
