

Introduction: When Prescriptions Tell a National Story
Prescription data are more than administrative records; they are epidemiological fingerprints. When analyzed longitudinally, they reveal how a population ages, how clinicians adapt to evolving evidence, and how patients’ expectations shift over time. The Norwegian study published in European Urology Open Science provides precisely this perspective: a nationwide evaluation of prescription trends for male lower urinary tract symptoms (LUTS), benign prostatic hyperplasia (BPH), erectile dysfunction (ED), and urinary incontinence from 2004 to 2020 .
Unlike many countries that rely on insurance claims or fragmented datasets, Norway benefits from a centralized electronic prescribing system. Every prescription dispensed at every pharmacy is recorded in the Norwegian Prescription Database (NorPD). This infrastructure transforms routine prescribing into a powerful public health observatory.
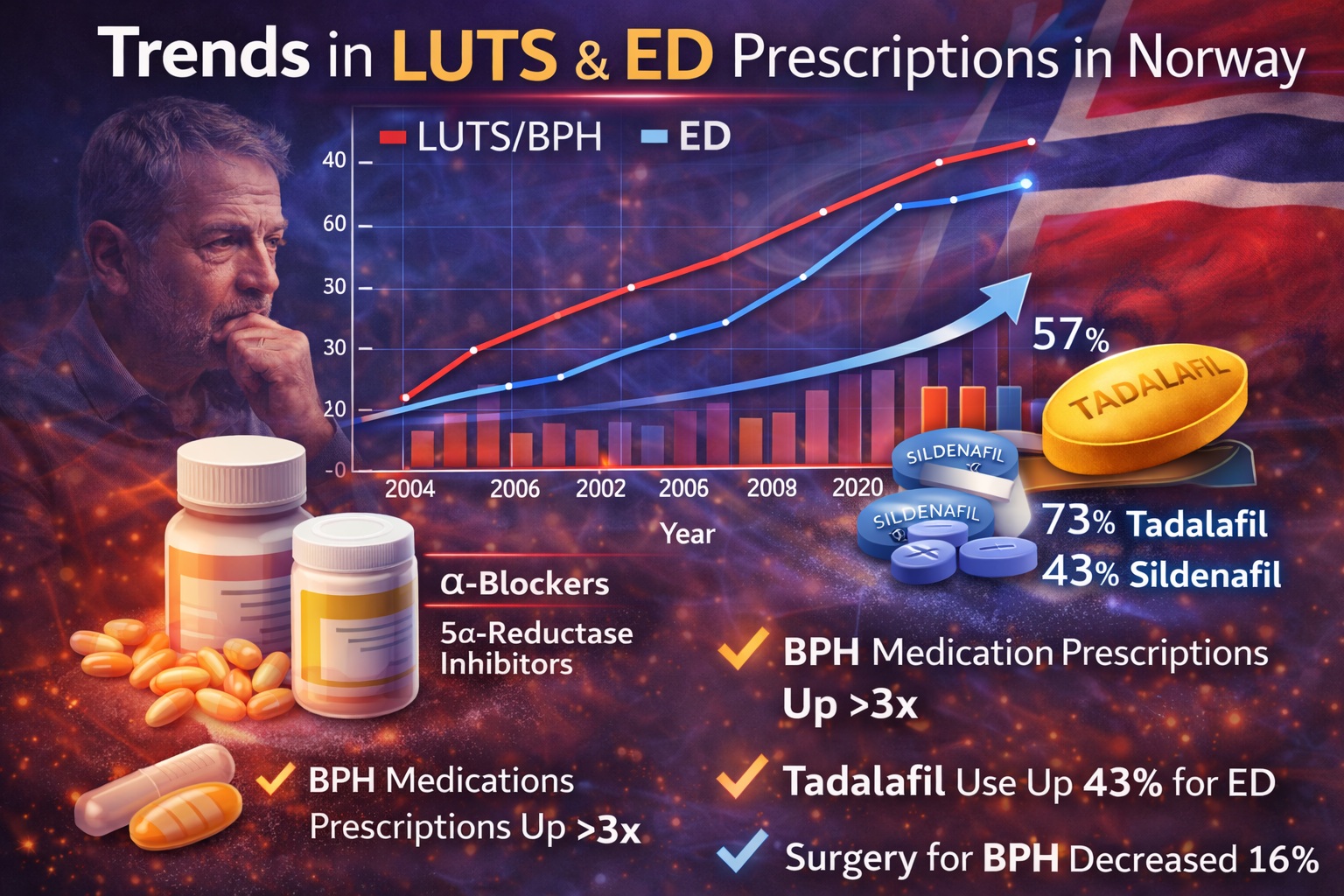
The results are striking. Prescriptions for BPH, ED, and incontinence medications have all increased substantially over two decades. BPH pharmacotherapy, in particular, has surged dramatically. ED medications, including tadalafil, have shown consistent growth, though with nuanced shifts in market distribution. Meanwhile, surgical volumes for BPH have paradoxically declined.
This article synthesizes the findings and explores their broader clinical implications. We will examine what these prescription trends reveal about demographic change, therapeutic priorities, healthcare policy, and the evolving place of tadalafil in urological practice.
Methodological Strength: The Power of a Centralized Prescription Database
The study employed a retrospective observational design using NorPD data from 2004 to 2020 . Medications were classified using the Anatomical Therapeutic Chemical (ATC) system, enabling systematic identification of:
- BPH medications (G04C)
- Urinary incontinence/frequency medications (G04BD)
- Erectile dysfunction medications (G04BE)
This classification approach ensures consistency across years and eliminates coding ambiguity. Importantly, because all prescriptions in Norway are electronic, data completeness is exceptional.
The study also integrated surgical data for BPH from 2016 to 2023 via the Norwegian Patient Register. This dual perspective—medical and surgical—allows for a rare comparison between pharmacotherapy expansion and operative trends.
Statistical analysis using Poisson regression confirmed significant upward trends across medication categories. The robustness of the data source is arguably the study’s greatest strength. In a world of fragmented healthcare datasets, Norway offers near-total visibility.
BPH Pharmacotherapy: A Threefold Increase and a Demographic Signal
The most dramatic trend was observed in medications for benign prostatic hyperplasia.
Between 2004 and 2020, total annual BPH prescriptions increased from 23,711 to 102,531 . By 2020, 38 per 1000 men were receiving a BPH medication—a 3.6-fold increase over the study period.
The average annual increase in users was 8.9% (p < 0.001). Among men aged 75 years, one in ten received a prescription for BPH medication in 2020. By contrast, only seven per 1000 men aged 40–49 were treated.
Alpha-adrenoceptor antagonists were prescribed five times more often than 5-alpha reductase inhibitors. Combination therapies, such as tamsulosin-dutasteride, showed gradual uptake following introduction.
The demographic explanation is straightforward: Norway’s population aged substantially over the study period. Life expectancy increased, and the proportion of men aged 67–79 and 80–89 expanded significantly .
Yet demographics alone do not explain a tripling in prescriptions. Cultural and professional shifts are also at play. Increasing management of LUTS in primary care likely contributes to expanded pharmacotherapy.
Erectile Dysfunction Medications: Growth, Stabilization, and the Role of Tadalafil
ED medication use also increased significantly, though at a slower pace than BPH medications.
The number of users per 1000 men rose from 4.4 to 19 over the study period, with an average annual increase of 4.7% (p < 0.001) .
By 2020:
- Sildenafil accounted for 47% of prescriptions
- Tadalafil accounted for 43%
- Vardenafil accounted for 4.8%
The near parity between sildenafil and tadalafil is notable. Tadalafil, with its longer half-life and 36-hour therapeutic window, offers greater flexibility and spontaneity compared with shorter-acting agents.
In men aged 65–74, one in ten received an ED prescription. Even in men aged 40–49, four in 100 were prescribed ED medication.
Interestingly, prescriptions for sildenafil declined toward the end of the study period, likely due to its over-the-counter availability from 2019 onward . This regulatory change artificially reduced prescription numbers without necessarily reducing use.
Another factor influencing 2020 data may have been the COVID-19 pandemic. Reduced social contact plausibly dampened ED medication demand during that year.
Nevertheless, tadalafil’s sustained growth suggests stable clinician confidence in its efficacy and tolerability.
Urinary Incontinence and Overactive Bladder: Mirabegron’s Ascendancy
Medications for urinary incontinence and urgency increased from 4.4 to 9.3 users per 1000 men over the study period . The average annual increase was 5.8%.
By 2020:
- Mirabegron accounted for 62% of prescriptions
- Oxybutynin accounted for 17%
- Fesoterodine accounted for 9%
A particularly important observation was the decline in oxybutynin use among elderly men. Awareness of its cognitive adverse effects likely drove prescribers toward mirabegron, a beta-3 agonist with a more favorable central nervous system profile.
Men aged 80–90 had the highest prescription rates. Approximately 10 in 200 men in this age group were treated.
While women still received more prescriptions overall, the male prescription rate increased more rapidly, narrowing the female-to-male ratio over time .
Surgical Volume Decline: Are We Postponing the Inevitable?
Perhaps the most intriguing finding is the decline in BPH surgical volume between 2016 and 2023.
Total BPH surgeries decreased by 16% during this period . Transurethral resection of the prostate (TURP) remained dominant, accounting for 92% of cases in 2023.
No compensatory increase in alternative minimally invasive procedures was observed.
This divergence—rising medication prescriptions and declining surgery—raises an important question: are we preventing surgery or merely postponing it?
Pharmacotherapy may delay intervention. However, prolonged obstruction can lead to bladder dysfunction, recurrent retention, and renal impairment. If medication only defers surgery, a future surge in demand could strain surgical capacity.
Longitudinal patient-level studies are required to determine conversion rates from medical to surgical therapy.
Health Policy and Economic Considerations
Prescription trends do not exist in isolation; they reflect healthcare policy.
Mirabegron, for example, is heavily subsidized in Norway when clinical criteria are met. Cost-sharing structures influence prescribing behavior.
Similarly, tadalafil’s positioning relative to sildenafil may be shaped by reimbursement rules and patient preferences.
Centralized electronic prescribing also facilitates adherence monitoring and national cost oversight.
The Norwegian model illustrates how health systems with comprehensive databases can monitor treatment diffusion in real time.
Cultural Shifts: ED as a Quality-of-Life Condition
The steady rise in ED prescriptions reflects more than demographic change. It signals evolving attitudes toward male sexual health.
Two decades ago, ED often remained unspoken. Today, it is recognized as a quality-of-life condition deserving medical attention.
Tadalafil’s strong uptake underscores its acceptance not only as a pharmacologic solution but as a lifestyle-enabling therapy. Its extended duration and food-independent pharmacokinetics align with modern expectations of flexibility.
Furthermore, increased radical prostatectomy rates and penile rehabilitation strategies may have heightened awareness of ED treatment options.
Strengths and Limitations
The study’s principal strength lies in its national coverage. NorPD captures every dispensed prescription in Norway .
However, limitations include:
- Absence of data on prescribing specialty
- No information on adherence or discontinuation
- Lack of linkage between prescription and surgical outcomes
Despite these limitations, the dataset provides a robust macro-level view of therapeutic evolution.
Clinical Implications: What Should Practitioners Take Away?
Several practical lessons emerge:
First, pharmacotherapy for LUTS and ED is expanding rapidly. Clinicians should anticipate increased patient demand.
Second, tadalafil has secured a strong position alongside sildenafil, reflecting durable clinician confidence.
Third, declining surgical volumes do not necessarily equate to disease control. Monitoring long-term outcomes is essential.
Finally, aging populations will continue to drive urological medication demand. Health systems must plan accordingly.
Conclusion: A Nation Aging, Prescribing, and Reframing Male Health
Between 2004 and 2020, Norway witnessed a substantial rise in prescriptions for BPH, ED, and urinary incontinence medications . BPH pharmacotherapy expanded most dramatically. ED prescriptions grew steadily, with tadalafil emerging as a co-dominant agent alongside sildenafil.
Simultaneously, BPH surgical volumes declined. Whether this reflects true disease control or delayed intervention remains uncertain.
The data tell a broader story: male urological health is increasingly managed pharmacologically. As populations age and stigma diminishes, medications such as tadalafil are likely to remain central in therapeutic strategies.
Prescription databases, when analyzed thoughtfully, provide more than statistics—they reveal the direction of modern medicine.
FAQ
1. Why have prescriptions for BPH medications increased so dramatically?
The rise reflects population aging, increased primary care management of LUTS, and broader acceptance of pharmacotherapy as first-line treatment. In Norway, one in ten men aged 75 now receives BPH medication.
2. How significant is tadalafil’s role in ED treatment nationally?
By 2020, tadalafil accounted for 43% of ED prescriptions in Norway, nearly matching sildenafil. Its long half-life and flexible dosing make it a widely preferred option.
3. Does the decline in BPH surgery mean medications are curing the condition?
Not necessarily. Surgical volume has decreased, but it remains unclear whether pharmacotherapy prevents surgery or merely postpones it. Long-term patient-level studies are needed to clarify this relationship.
