

Introduction
Radical prostatectomy (RP) remains a cornerstone of curative therapy for localized prostate cancer. While oncological outcomes are excellent—with survival rates approaching 100% for organ-confined disease—the functional cost is high. Erectile dysfunction (ED) after RP is one of the most feared complications, reported in up to 87% of men despite modern nerve-sparing and robotic techniques. For many patients, loss of erectile function profoundly impacts quality of life, intimate relationships, and psychological well-being.
This clinical challenge has given rise to the concept of penile rehabilitation (PR)—an intervention strategy aiming not just to treat ED but to preserve erectile tissue integrity and promote recovery of spontaneous function. Among available pharmacotherapies, phosphodiesterase type 5 inhibitors (PDE5i) are the foundation of most PR protocols. They are safe, effective, and widely used.
Within this class, tadalafil holds particular promise due to its long half-life and unique antifibrotic effects. This article examines the scientific rationale, preclinical and clinical evidence, and ongoing controversies surrounding tadalafil as a key tool in post-prostatectomy penile rehabilitation.
Pathophysiology of Erectile Dysfunction After Radical Prostatectomy
Understanding post-RP ED requires an appreciation of the complex physiology of erection. Normal function depends on the interplay of vascular inflow, neural signaling, and cavernosal smooth muscle relaxation. Any disruption of these pathways jeopardizes erectile performance.
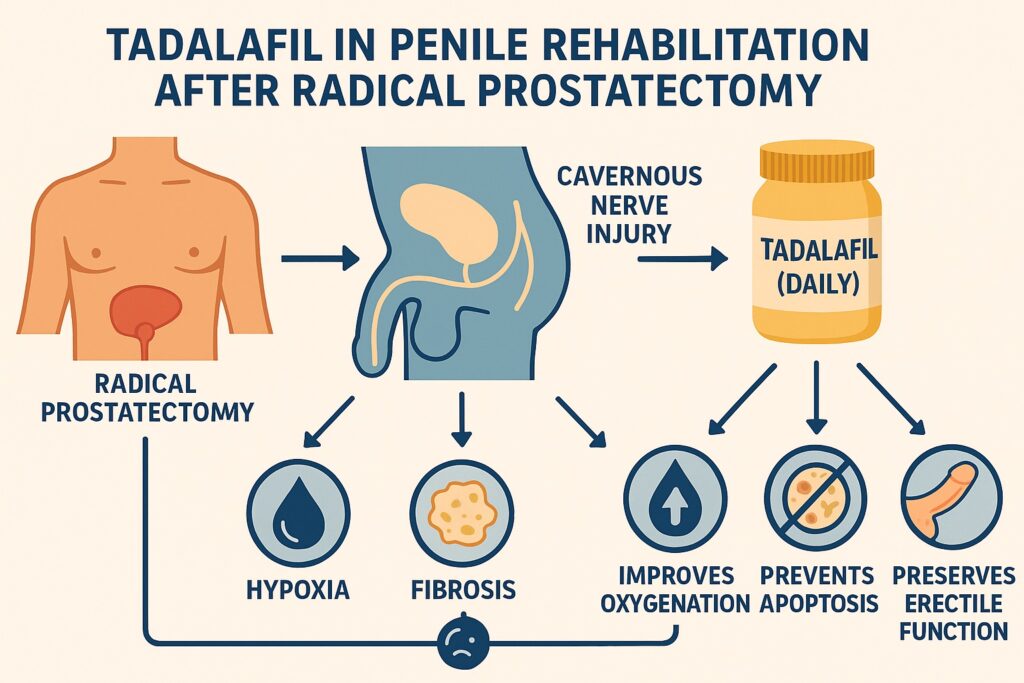
During RP, even with nerve-sparing techniques, cavernous nerves are vulnerable to traction, thermal injury, or transection. Loss of neuronal nitric oxide synthase (nNOS) reduces nitric oxide (NO) availability, impairing smooth muscle relaxation and nocturnal erections. The absence of these physiological erections leads to chronic cavernosal hypoxia.
Hypoxia triggers a cascade of pathological events:
- Upregulation of pro-fibrotic mediators such as transforming growth factor-β and endothelin-1
- Increased apoptosis of cavernosal smooth muscle cells
- Excess collagen deposition and corporal fibrosis
- Loss of compliance and veno-occlusive dysfunction
Ultimately, the penis undergoes structural remodeling, shifting from a dynamic erectile organ to a fibrotic, noncompliant structure incapable of erection. Preventing this hypoxia-fibrosis-apoptosis cycle is the rationale for early penile rehabilitation.
Mechanisms of Action: Why Tadalafil?
Tadalafil is a potent and selective PDE5 inhibitor. Its unique features make it attractive in PR strategies.
- Pharmacokinetics: With a half-life of 17.5 hours, tadalafil provides therapeutic levels for up to 36 hours. This prolonged window enhances spontaneity and may sustain cavernosal oxygenation.
- Tissue Effects: Animal studies demonstrate tadalafil preserves smooth muscle content, increases smooth muscle-to-collagen ratio, and reduces apoptosis. Activation of survival kinases (Akt, ERK 1/2) supports cell survival pathways.
- Clinical Utility: Unlike sildenafil, tadalafil’s absorption is not significantly affected by food, simplifying daily dosing regimens.
Thus, tadalafil may not only enhance penile hemodynamics acutely but also protect cavernosal architecture chronically, offering a dual role in both therapy and prevention.
Evidence from Preclinical Studies
Animal models of cavernous nerve injury have been instrumental in demonstrating tadalafil’s protective role.
Kovanecz et al. showed that 45 days of daily tadalafil in rats with bilateral nerve resection restored intracavernosal pressure, preserved smooth muscle, and reduced apoptosis. Similarly, Lysiak et al. observed that tadalafil increased phosphorylation of pro-survival kinases and reduced apoptotic cell numbers up to six weeks after injury.
These findings highlight tadalafil’s antifibrotic and antiapoptotic mechanisms, making it unique among PDE5 inhibitors for long-term tissue preservation.
Clinical Trials: Tadalafil After Radical Prostatectomy
Several well-designed studies have evaluated tadalafil in post-RP populations.
- Montorsi et al. (2004): A randomized placebo-controlled trial of 303 men after bilateral nerve-sparing RP found that on-demand tadalafil significantly improved IIEF scores compared to placebo after 12 weeks. No serious adverse events were reported.
- Montorsi et al. (2014, REACTT trial): In a multicenter, three-arm study (n=423), patients received tadalafil daily, on-demand, or placebo for nine months. Daily tadalafil significantly improved rates of erectile function recovery (IIEF-EF ≥22) compared with placebo. Importantly, penile length preservation was observed in the daily group, but not with on-demand use. After washout, the advantage diminished, suggesting that continuous therapy is required to maintain benefit.
- Seo et al. (2014): In 92 men undergoing robotic RP, daily tadalafil 5 mg for one year significantly improved IIEF scores compared to placebo, with benefits evident across all functional domains.
Collectively, these trials underscore the superiority of daily tadalafil over on-demand dosing in the rehabilitation setting, particularly in terms of preserving penile structure and function.
Daily vs On-Demand Tadalafil: A Critical Comparison
The distinction between daily low-dose therapy and on-demand higher-dose therapy is crucial.
Daily tadalafil ensures continuous PDE5 inhibition, maintaining basal cavernosal oxygenation and preventing fibrosis. This strategy aligns with the mechanistic rationale of PR, which emphasizes prevention of hypoxia-induced injury rather than episodic correction.
On-demand therapy improves erections when taken, but its intermittent nature may not prevent structural deterioration. Evidence from REACTT supports this: penile length preservation was significant only in the daily tadalafil group.
Therefore, for true penile rehabilitation, daily dosing appears superior, though patient adherence and cost remain challenges.
Factors Influencing Outcomes
Success of tadalafil in PR depends on multiple variables:
- Nerve-Sparing Status: Bilateral nerve-sparing RP offers the greatest chance of recovery; outcomes decline significantly with unilateral or non-nerve-sparing surgery.
- Age and Baseline Erectile Function: Younger men with good preoperative erectile function respond better.
- Surgical Technique: Emerging data suggest intrafascial nerve-sparing and robotic approaches may enhance recovery, though definitive evidence is lacking.
- Duration of Therapy: Longer courses correlate with better outcomes; some suggest up to 4 years of therapy may be beneficial in nerve-sparing patients.
Safety and Tolerability
Tadalafil is generally well tolerated. The most common side effects are headache, flushing, dyspepsia, nasal congestion, and back pain. Rates of discontinuation due to adverse events are low. Importantly, no increase in serious adverse events has been reported in post-RP populations.
Given the devastating psychological toll of ED, the favorable safety profile strongly supports tadalafil as a reasonable first-line choice.
Remaining Controversies
Despite encouraging evidence, several debates persist:
- Optimal timing: Should tadalafil be started immediately postoperatively, or even preoperatively, to maximize benefit? Animal studies favor early initiation, but clinical data remain inconclusive.
- Duration of therapy: How long should daily therapy continue? Some propose prolonged use, yet cost and adherence are barriers.
- Endpoints: Many trials use IIEF as the primary outcome, but preservation of penile length and cavernosal architecture may be equally important.
Ultimately, large, multicenter, randomized controlled trials with long-term follow-up are needed before universal guidelines can be solidified.
Conclusion
Erectile dysfunction after radical prostatectomy remains a prevalent and distressing complication. Tadalafil, with its long half-life, antifibrotic properties, and favorable safety profile, has emerged as a cornerstone in penile rehabilitation strategies. Evidence supports daily use as superior to on-demand therapy, particularly in preserving penile tissue and length.
While definitive protocols await further validation, the current data justify tadalafil as the first-line pharmacological agent for ED rehabilitation post-RP. For patients and partners navigating the dual challenges of cancer survival and sexual recovery, tadalafil offers not just improved erections but the possibility of restored confidence, intimacy, and quality of life.
FAQ
1. Is tadalafil better than sildenafil for post-prostatectomy ED?
Yes, in the context of penile rehabilitation. Tadalafil’s longer half-life and continuous action provide advantages in preserving penile tissue and promoting spontaneous recovery, while sildenafil is typically used for episodic treatment.
2. Should tadalafil be taken daily or on-demand after surgery?
Evidence favors daily tadalafil (5 mg) for penile rehabilitation, as it maintains tissue oxygenation and prevents fibrosis. On-demand use helps with erections but does not appear to protect long-term penile structure.
3. How long should penile rehabilitation with tadalafil continue?
There is no consensus. Some studies suggest benefits with therapy up to 12 months, while others propose extending use to several years in men with nerve-sparing surgery. Duration should be individualized.
