

Benign prostatic hyperplasia (BPH) rarely arrives alone. It brings obstruction, irritative urinary symptoms, sexual dysfunction, frustration, and — not infrequently — therapeutic disappointment. For many men, especially those previously treated without success, the experience of BPH becomes less about urinary flow and more about quality of life. Weak stream may be tolerable; urgency at 3 a.m., less so. And sexual dysfunction layered on top of it all often becomes the decisive factor in adherence or abandonment of therapy.
Recent evidence has explored a pharmacological strategy that may finally address the triad of obstruction, bladder hyperactivity, and sexual function simultaneously. The combined administration of dutasteride, tadalafil, and solifenacin represents a rational attempt to treat the prostate, the bladder, and erectile physiology in parallel. The question is not whether each drug works independently — that is well established. The real question is whether their simultaneous use can produce clinically meaningful synergy without unacceptable adverse effects.
This article examines the clinical logic, therapeutic impact, and practical implications of triple combination therapy in men with previously unsuccessful treatment outcomes.
The Clinical Problem: When BPH Is More Than Obstruction
BPH has long been defined by prostate enlargement and bladder outlet obstruction. However, modern urology recognizes that lower urinary tract symptoms (LUTS) are multifactorial. Mechanical compression from prostatic enlargement explains only part of the clinical picture. Bladder hyperactivity, detrusor hypoxia, altered nitric oxide signaling, increased Rho-kinase activity, and pelvic microvascular changes all contribute to symptom burden.
Patients commonly report:
- Weak urinary stream, straining, incomplete emptying
- Urgency, frequency, nocturia
- Reduced libido, erectile dysfunction, ejaculatory disturbance
These symptoms are not independent phenomena. Obstruction may coexist with detrusor overactivity. Sexual dysfunction may be exacerbated by both the disease and its treatment. Emotional distress, reduced self-esteem, and reactive depressive symptoms frequently follow.
Traditional monotherapy often fails because it targets only one element of the pathophysiological cascade. Alpha-blockers relieve dynamic obstruction but do not shrink the prostate. 5-alpha-reductase inhibitors reduce prostate volume but require months to act and may impair sexual function. Antimuscarinics address irritative symptoms but risk urinary retention if obstruction persists. PDE5 inhibitors improve erectile function and may modestly influence LUTS, yet they are not primarily anti-obstructive agents.
When therapy addresses only one node of this network, clinical dissatisfaction is predictable.
Pharmacological Rationale for Triple Therapy
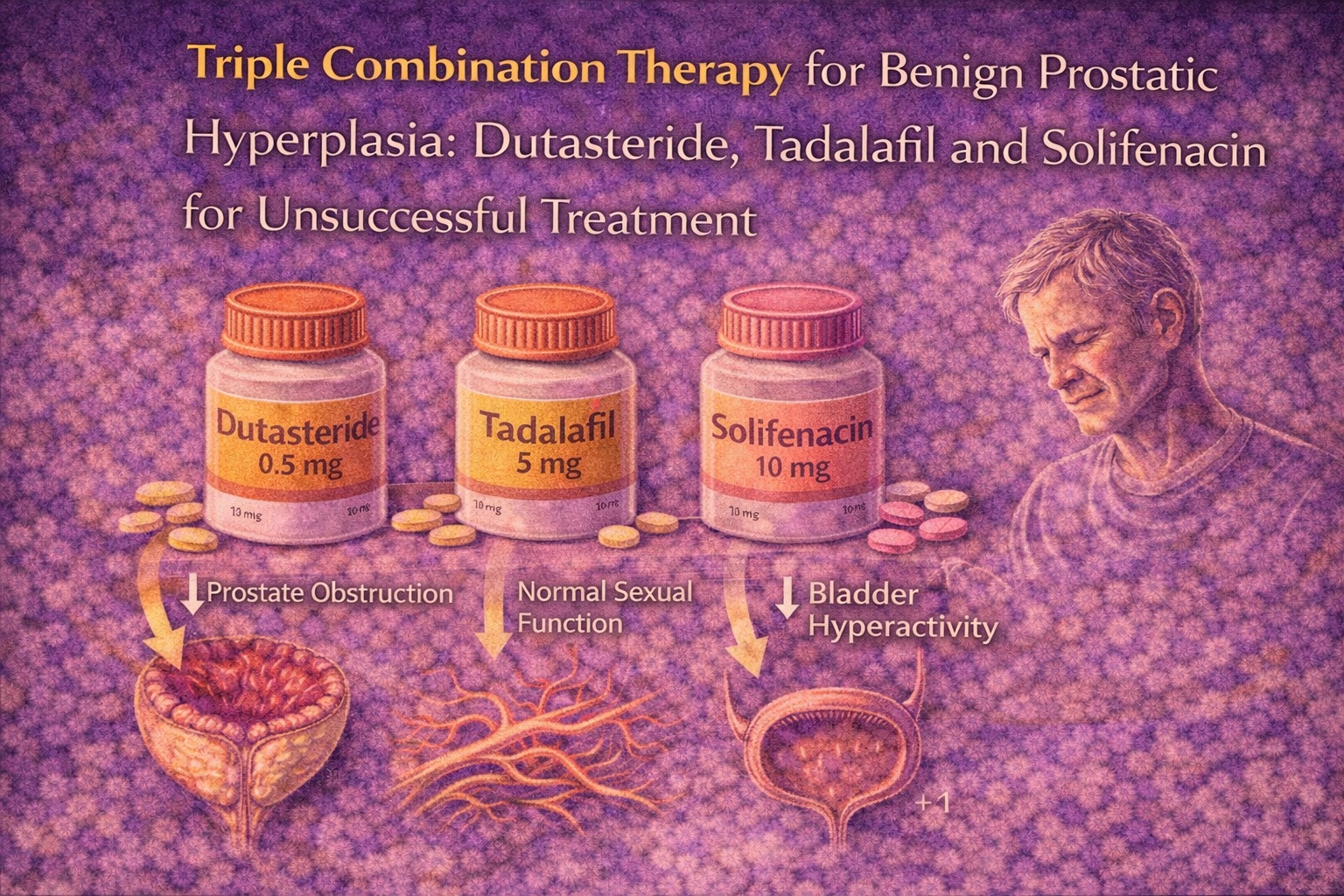
The rationale for combining dutasteride, tadalafil, and solifenacin rests on complementary mechanisms.
Dutasteride, a dual 5-alpha-reductase inhibitor, suppresses conversion of testosterone to dihydrotestosterone (DHT), leading to gradual prostate shrinkage and reduced mechanical obstruction. It targets structural progression of BPH. However, its sexual side effects — reduced libido, erectile dysfunction, ejaculatory disturbance — are well documented.
Tadalafil, a phosphodiesterase-5 inhibitor, enhances nitric oxide-mediated vasodilation and improves erectile function. It also influences smooth muscle tone within the lower urinary tract and may improve perfusion of pelvic tissues. Importantly, it can counteract the sexual adverse effects of dutasteride.
Solifenacin, an antimuscarinic agent, reduces detrusor overactivity by blocking M3 receptors. It specifically targets urgency, frequency, and nocturia — symptoms that often drive patients to seek care.
The conceptual elegance of triple therapy lies in division of labor:
- Dutasteride reduces prostate size.
- Solifenacin calms the bladder.
- Tadalafil preserves (and potentially enhances) sexual function.
It is, in effect, a strategy designed not merely to improve urinary flow but to preserve dignity and adherence.
Study Design and Patient Population
The clinical evaluation of this approach involved men with BPH accompanied by both obstructive and overactive bladder symptoms who had previously experienced unsatisfactory treatment outcomes .
Nearly 300 men were randomized into three treatment arms, each receiving dutasteride 0.5 mg daily, with varying doses of tadalafil and solifenacin:
- Low-dose combination
- Standard-dose combination
- High-dose combination
The primary endpoint was assessed at 12 weeks, with secondary attention to the speed of symptom improvement. Validated instruments were used:
- International Prostate Symptom Score (I-PSS)
- Overactive Bladder Questionnaire (OAB-q)
- International Index of Erectile Function (IIEF)
- Male Sexual Health Questionnaire (MSHQ-EjD)
- Uroflowmetry
The inclusion of both subjective questionnaires and objective flow measurements strengthens internal validity. Importantly, the population consisted of patients previously dissatisfied with therapy — a clinically relevant group often underrepresented in trials.
Effects on Obstructive Symptoms
Across groups receiving standard and elevated doses, significant improvement in obstructive symptoms was observed.
Mean I-PSS scores decreased substantially, and uroflowmetry parameters (including maximum flow rate) improved meaningfully. These changes align with the known pharmacodynamics of dutasteride, which requires several weeks to reduce DHT levels and induce prostate shrinkage.
Interestingly, improvement was more pronounced in standard- and high-dose groups than in the low-dose group. This suggests that while dutasteride acts as the structural backbone of therapy, adjunct agents may contribute indirectly — possibly through improved detrusor function and pelvic perfusion.
Importantly, obstructive improvement occurred gradually, reflecting the biological timeline of prostate remodeling. Patients and clinicians must understand that structural change cannot be rushed, even if irritative symptoms can.
Rapid Suppression of Hyperactivity Symptoms
The most clinically striking result involved bladder hyperactivity.
In the high-dose group, significant reductions in urgency, nocturia, and daytime frequency were evident as early as four weeks. This rapid response contrasts with the slower timeline typically associated with monotherapy.
The standard-dose group also demonstrated improvement, though more gradually. The low-dose regimen failed to produce clinically meaningful change.
This finding carries practical importance. Irritative symptoms — especially nocturia and urgency — disproportionately affect quality of life. Rapid improvement may strengthen patient motivation and adherence. In clinical reality, a patient who sleeps through the night is far more likely to continue therapy than one who is told to “wait three months.”
The study suggests that sufficient antimuscarinic dosing is necessary to achieve early symptomatic control without compromising safety.
Sexual Function: Preservation Versus Enhancement
Perhaps the most delicate aspect of BPH management is sexual function.
Dutasteride monotherapy is associated with measurable reductions in libido and erectile performance. This effect frequently leads to discontinuation. The inclusion of tadalafil was therefore not cosmetic but strategic.
In the standard-dose group, sexual function remained stable. In the high-dose group, erectile and satisfaction domains improved significantly over baseline. This improvement became evident around eight weeks.
This finding is clinically meaningful. It demonstrates not only protection against dutasteride-induced decline but potential net gain in sexual performance. Such an outcome redefines patient counseling. Instead of apologizing for side effects, clinicians may reasonably frame therapy as function-preserving.
The low-dose group, again, did not demonstrate robust improvement.
Safety Profile and Tolerability
Combination therapy inevitably raises concerns regarding cumulative adverse effects. However, the incidence of side effects remained within expected ranges .
Reported adverse effects included:
- Dry mouth
- Headache
- Mild dizziness
- Occasional nausea
Most were transient and did not necessitate discontinuation. Severe events were uncommon. Notably, even higher doses of tadalafil and solifenacin did not produce disproportionate toxicity.
This absence of additive harm supports the pharmacological compatibility of the regimen. Importantly, no signal suggested increased urinary retention — a theoretical concern when combining antimuscarinics with obstructive pathology.
Clinical Interpretation and Behavioral Implications
Therapeutic success in BPH extends beyond symptom scores. It influences patient psychology and adherence behavior.
Men who previously abandoned therapy often cite three reasons:
- Slow onset of benefit
- Persistent irritative symptoms
- Sexual side effects
Triple therapy addresses all three simultaneously. Rapid suppression of urgency enhances early satisfaction. Preservation or improvement of sexual function reduces anxiety. Gradual improvement in flow confirms structural efficacy.
The behavioral consequence may be improved medication adherence. Although adherence was not directly measured, the pattern of symptom evolution strongly suggests improved retention potential.
There is, admittedly, a quiet irony here: three drugs may produce better simplicity in outcomes than one drug alone.
Limitations and Areas for Future Research
Despite promising results, limitations deserve recognition.
The observation period was relatively short. Long-term sustainability beyond 12 weeks requires further evaluation. Additionally, patients with severe comorbidities were excluded; generalizability to frail elderly populations remains uncertain.
The study did not directly measure long-term sexual satisfaction trajectories or psychological outcomes. Nor did it compare triple therapy against surgical intervention.
Future research should explore:
- 6- to 12-month outcomes
- Impact on medication adherence
- Comparative effectiveness versus minimally invasive surgery
- Cost-effectiveness analysis
Nonetheless, the current data provide compelling short-term evidence of safety and efficacy.
Practical Implications for Clinical Practice
For men with moderate-to-severe BPH accompanied by hyperactivity symptoms and concerns about sexual function, triple therapy offers a rational option.
Standard dosing may suffice for gradual improvement while maintaining sexual function. Higher doses of solifenacin and tadalafil may be considered when rapid symptom control is clinically desirable and tolerability permits.
Patient selection remains critical. Those with significant post-void residual volume or high risk of urinary retention require careful monitoring.
Most importantly, therapy should be individualized. The goal is not polypharmacy for its own sake but targeted pharmacological synergy.
Conclusion
Simultaneous administration of dutasteride, tadalafil, and solifenacin represents a coherent, mechanism-based strategy for men with BPH who experience obstruction, bladder hyperactivity, and vulnerability to sexual dysfunction.
Standard dosing provides gradual improvement without sexual compromise. Higher dosing accelerates relief of irritative symptoms and may enhance erectile function without substantially increasing adverse events.
In an era where patient satisfaction and adherence define real-world success, triple combination therapy may represent not therapeutic excess, but therapeutic precision.
FAQ
1. Is triple therapy safe for long-term use?
Short-term data demonstrate acceptable tolerability. Most side effects are mild and transient. Long-term safety beyond 12 weeks requires further study, but current pharmacological profiles of each agent are well established.
2. Does tadalafil completely prevent sexual side effects of dutasteride?
Evidence suggests it prevents deterioration and may improve erectile function at adequate doses. However, individual responses vary, and counseling should remain realistic.
3. Who is the ideal candidate for this combination?
Men with moderate-to-severe BPH, persistent overactive bladder symptoms, prior unsuccessful monotherapy, and concerns regarding sexual function represent the most appropriate candidates.
