

Introduction
For decades, the pathophysiology of lower urinary tract symptoms (LUTS) associated with benign prostatic hyperplasia (BPH) was simplistically viewed as a mechanical problem—a matter of urethral compression and static obstruction. Yet clinical observations consistently contradicted this narrow view. Not all prostates that enlarged caused symptoms, and not all symptomatic men benefited from 5α-reductase inhibitors or α-blockers alone.
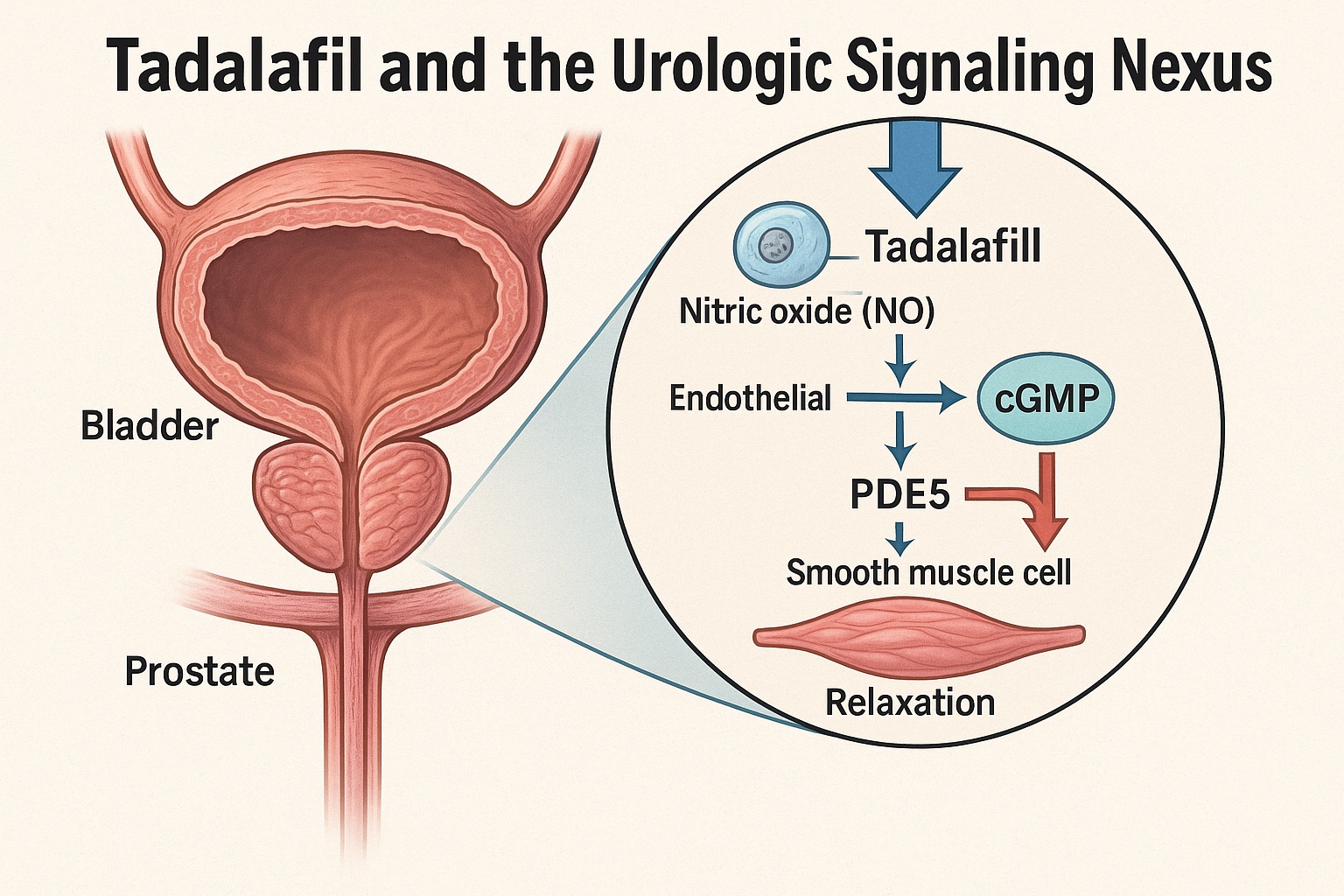
Modern understanding now acknowledges LUTS/BPH as a complex interplay between smooth muscle tone, vascular dynamics, autonomic regulation, and inflammation, extending well beyond the gland itself. Among the pharmacologic agents that have reframed this understanding is tadalafil, a selective phosphodiesterase type-5 (PDE5) inhibitor. Originally developed to enhance penile hemodynamics, tadalafil has revealed broader urologic effects rooted in NO–cGMP–PKG signaling, endothelial repair, and detrusor relaxation.
This article delves into the pathophysiologic rationale and pharmacologic mechanisms through which tadalafil exerts its effects on LUTS/BPH. The focus lies not on its sexual pharmacodynamics but on its molecular finesse within the bladder–prostate–pelvic vascular axis, a domain where urology meets vascular physiology and smooth muscle biology.
The Pathophysiology of LUTS/BPH: More Than Just an Obstruction
LUTS/BPH represents a multifactorial condition integrating static, dynamic, and neuromodulatory components. The static component arises from hyperplastic growth within the prostatic transition zone, increasing urethral resistance. The dynamic component—mediated primarily by α1-adrenergic tone—reflects smooth muscle contractility within the prostate, bladder neck, and urethra. Yet neither fully explains symptom severity, which correlates weakly with prostate size.
Contemporary studies have illuminated a third dimension: the pelvic vascular contribution. Aging, diabetes, and endothelial dysfunction reduce nitric oxide (NO) bioavailability, leading to ischemia of the lower urinary tract. Hypoxia triggers smooth muscle hyperactivity, collagen deposition, and oxidative stress, all of which amplify obstruction. Simultaneously, impaired blood flow compromises the relaxation phase of micturition and may contribute to detrusor overactivity.
In this context, agents that restore endothelial NO signaling and normalize cGMP-dependent smooth muscle relaxation are not merely adjuncts—they address a root defect in LUTS pathophysiology.
PDE5 in the Lower Urinary Tract: Mapping the Molecular Landscape
PDE5, once thought to be confined to the corpus cavernosum, is now known to be abundantly expressed throughout the bladder neck, prostate stroma, and pelvic vasculature. Immunohistochemical analyses show localization in smooth muscle cells, endothelial cells, and nerve terminals of the lower urinary tract.
The enzyme’s role is pivotal: it hydrolyzes cyclic guanosine monophosphate (cGMP), the second messenger of the NO signaling cascade. By breaking down cGMP, PDE5 effectively terminates protein kinase G (PKG) activation, curtailing downstream relaxation signals. The result is sustained smooth muscle tone, reduced blood flow, and impaired tissue oxygenation.
Tadalafil’s high selectivity for PDE5 (IC₅₀ ≈ 5 nM) and prolonged half-life (≈17 hours) make it ideal for continuous modulation of this pathway. By inhibiting PDE5, tadalafil elevates intracellular cGMP levels, enhancing PKG activity, and ultimately reducing calcium influx through L-type Ca²⁺ channels. The downstream effect is smooth muscle relaxation in the prostate, bladder neck, and associated vasculature.
Nitric Oxide and cGMP Signaling in Urologic Function
The NO–cGMP pathway orchestrates both penile erection and urinary tract function. In the prostate and bladder, neuronal NO synthase (nNOS) and endothelial NO synthase (eNOS) generate NO, which diffuses into adjacent smooth muscle cells. There, it stimulates soluble guanylate cyclase (sGC) to convert GTP into cGMP.
cGMP activates PKG, which phosphorylates several effector proteins that modulate intracellular calcium homeostasis, including:
- IP₃ receptors and phospholamban, reducing Ca²⁺ release from sarcoplasmic reticulum.
- Myosin light chain phosphatase, promoting dephosphorylation of myosin and relaxation.
- RhoA/Rho-kinase pathway suppression, mitigating sustained smooth muscle contraction.
By preserving this signaling integrity, tadalafil counteracts the hypercontractile state induced by aging, hypoxia, or sympathetic overactivity. The result is improved bladder outflow and reduction of irritative symptoms such as frequency and urgency—effects verified by multiple mechanistic and clinical studies.
Endothelial Dysfunction and Pelvic Hypoperfusion: The Hidden Link
One of the most underappreciated contributors to LUTS/BPH is chronic pelvic ischemia. Microvascular endothelial dysfunction in the prostatic and bladder arteries leads to reduced perfusion, causing oxidative stress and inflammation. Experimental models demonstrate that ischemic prostates exhibit fibromuscular hypertrophy, increased α1-adrenergic receptor density, and collagen deposition—all reversible with restoration of cGMP signaling.
Tadalafil, through PDE5 inhibition, exerts endothelium-restorative actions by several mechanisms:
- Augmenting NO bioavailability: cGMP-PKG activation enhances eNOS expression and limits oxidative NO degradation.
- Reducing inflammatory cytokines: Suppression of TNF-α and IL-6 mitigates chronic inflammatory infiltration.
- Promoting angiogenesis and microvascular repair: PKG signaling stimulates vascular endothelial growth factor (VEGF) pathways.
In human studies, tadalafil improved pelvic arterial flow and resistive indices measured by Doppler ultrasonography, supporting the hypothesis that part of its urologic efficacy derives from vascular rehabilitation rather than mere smooth muscle relaxation.
The Bladder Connection: Detrusor Modulation and Afferent Control
While prostatic relaxation improves voiding, tadalafil’s influence extends to the detrusor muscle and bladder sensory pathways. The bladder expresses both PDE5 and sGC, with cGMP signaling modulating detrusor tone and afferent sensitivity.
Tadalafil enhances detrusor compliance by reducing basal calcium levels and downregulating Rho-kinase activity, which otherwise maintains tonic contraction. In addition, by improving suburothelial blood flow, it stabilizes afferent nerve firing thresholds, leading to reduced urgency and frequency.
Animal models show that chronic PDE5 inhibition decreases bladder overactivity induced by outlet obstruction without impairing detrusor contractility. Translationally, this may explain why men treated with tadalafil often report not only better voiding but also fewer irritative symptoms—an effect distinct from α-blockers.
Tadalafil Pharmacodynamics: Beyond Penile Vasodilation
Tadalafil’s pharmacologic identity is defined by high potency, tissue selectivity, and duration of action. It has a terminal half-life of 17.5 hours, enabling stable 24-hour PDE5 inhibition at once-daily doses of 5 mg. Its tissue distribution includes not only corpus cavernosum but also prostate, bladder, and vascular endothelium—a crucial distinction for LUTS/BPH efficacy.
The pharmacodynamic effects extend across three interrelated domains:
- Vasculature: Improved perfusion and oxygenation of pelvic organs.
- Smooth muscle: Reduced tone in prostate and bladder neck.
- Neural regulation: Modulated sensory afferent signaling, reducing urgency and frequency.
Unlike α-blockers, tadalafil does not cause orthostatic hypotension or retrograde ejaculation. Unlike 5α-reductase inhibitors, it acts rapidly without requiring glandular shrinkage. This unique combination—vasoprotective, neuromodulatory, and muscularly selective—makes it a pleiotropic regulator of lower urinary tract physiology.
Anti-Inflammatory and Anti-Fibrotic Mechanisms
Emerging evidence suggests that tadalafil’s benefits in LUTS/BPH also involve anti-inflammatory and anti-fibrotic signaling. The cGMP–PKG axis interferes with NF-κB activation, the transcriptional driver of cytokine release and fibrotic remodeling. In prostatic stromal cultures, PDE5 inhibition suppresses TGF-β1–induced collagen synthesis and smooth muscle proliferation.
Moreover, chronic tadalafil exposure reduces oxidized LDL and C-reactive protein levels, indicating systemic anti-inflammatory benefit. Such pleiotropy could theoretically decelerate the progressive fibromuscular remodeling that drives LUTS persistence despite conventional therapies.
Clinical Correlates: Mechanism Reflected in Outcome
In controlled clinical studies summarized by the World Journal of Men’s Health (2013) review, tadalafil 5 mg once daily consistently improved International Prostate Symptom Score (IPSS) by approximately −4 to −6 points relative to placebo. Interestingly, symptom improvement occurred without significant change in peak urinary flow rate (Qmax)—a finding that underscores its non-mechanical mode of action.
The symptomatic relief thus correlates more closely with functional restoration of bladder–prostate smooth muscle and vascular physiology than with luminal enlargement.
Furthermore, improvements in Erectile Function (IIEF) and Quality-of-Life (QoL) indices suggest tadalafil’s systemic vascular normalization—treating both penile and prostatic microcirculation via shared molecular pathways. The dual efficacy validates the mechanistic continuum between erectile and urinary dysfunction.
Pharmacologic Interactions and Safety Considerations
Tadalafil demonstrates a favorable safety profile in urologic populations. Unlike nonselective vasodilators, it does not significantly lower systemic blood pressure. The most common adverse events—headache, dyspepsia, back pain—are dose-related and generally mild.
Importantly, when combined with α1-blockers, tadalafil requires caution due to potential additive hypotension. However, when administered with tamsulosin 0.4 mg, studies reveal minimal hemodynamic interaction, making this combination clinically viable for dual symptom relief.
No significant hepatic or renal toxicities have been observed with chronic low-dose therapy, and long-term trials (up to one year) confirm stable hemodynamic and metabolic parameters. This tolerability supports tadalafil’s role as a continuous-action modulator rather than a symptomatic rescue drug.
Translational Implications: From Molecular Insight to Clinical Integration
The significance of tadalafil in LUTS/BPH transcends its numerical symptom reduction. Its mechanistic concordance with the underlying pathophysiology positions it as a disease-modifying adjunct—potentially slowing fibrotic remodeling and vascular decline.
Translationally, PDE5 inhibition offers a conceptual pivot from pressure-centric management (reducing obstruction) to signal-centric modulation (restoring physiologic homeostasis). This mirrors cardiology’s evolution from mechanical revascularization to endothelial repair.
In regions such as Asia, where metabolic syndrome and diabetes are highly prevalent among aging men, tadalafil’s vascular restorative properties carry even greater relevance. Improved endothelial function may concurrently mitigate cardiovascular risk, positioning daily PDE5 inhibition as a unifying strategy for both urologic and vascular health.
The Future: Integrating PDE5 Inhibitors in Urologic Precision Medicine
Future therapeutic frameworks may view tadalafil not merely as an ED agent but as a microvascular conditioner within the genitourinary system. Personalized application could involve stratifying patients based on biomarkers of endothelial dysfunction or pelvic ischemia—those most likely to benefit mechanistically.
Emerging imaging modalities, including contrast-enhanced ultrasound and functional MRI, can quantify prostatic perfusion and bladder wall oxygenation, offering objective endpoints for PDE5 therapy trials. Coupled with genomic insight into NOS3 and PDE5A polymorphisms, precision deployment of tadalafil may soon transform symptomatic management into molecular rehabilitation.
Conclusion
The traditional narrative of LUTS/BPH as a simple plumbing problem is obsolete. The condition represents a failure of integrated vascular, muscular, and neural homeostasis—a failure that tadalafil, through PDE5 inhibition, addresses with molecular precision.
By restoring NO–cGMP signaling, improving endothelial integrity, and reducing smooth muscle overactivity, tadalafil provides a unique pharmacologic bridge between erectile and urinary health. Its effects are not confined to symptom relief but extend to pathophysiologic correction, heralding a paradigm where urologic therapy aligns with vascular biology.
In essence, tadalafil does not merely “relax the prostate.” It re-educates the pelvic vasculature, recalibrates smooth muscle tone, and redefines how we understand LUTS/BPH at a molecular level. The transition from symptom suppression to signal restoration marks the evolution of urology from mechanical correction to biochemical precision.
FAQ
1. How does tadalafil differ mechanistically from α-blockers in LUTS/BPH?
Tadalafil targets the NO–cGMP–PKG signaling pathway, improving vascular perfusion and smooth muscle relaxation at a molecular level. α-blockers, in contrast, act directly on adrenergic receptors to reduce dynamic tone but do not address endothelial dysfunction or microvascular ischemia.
2. Does tadalafil actually reduce prostate size?
No. Tadalafil does not shrink the prostate. Its benefits stem from improved relaxation, oxygenation, and reduced inflammation, which alleviate symptoms without altering glandular volume.
3. Could tadalafil have disease-modifying potential in LUTS/BPH?
Yes. By restoring endothelial health and preventing fibrotic remodeling, long-term PDE5 inhibition may theoretically slow disease progression—a hypothesis currently under clinical exploration.
Primary reference:
Y. G. Lee et al. Urinary Tract Symptoms (LUTS) Secondary to BPH and LUTS/BPH with Erectile Dysfunction in Asian Men: A Systematic Review Focusing on Tadalafil. World Journal of Men’s Health, 2013; 31(3): 193–207.
