

Introduction: Erectile Dysfunction as a Vascular Mirror
Erectile dysfunction (ED) has long escaped the narrow confines of being viewed purely as a sexual ailment. In contemporary medicine, it is increasingly regarded as a systemic vascular disorder — an early sentinel of endothelial dysfunction and a clinical marker for underlying cardiovascular disease (CVD). The vascular endothelium, once thought to be a passive barrier, is now recognized as a dynamic endocrine organ regulating vascular tone, platelet aggregation, and smooth muscle proliferation through nitric oxide (NO) bioavailability. When the endothelium falters, the first organ to betray the imbalance is often the one most reliant on microvascular integrity: the penis.
The study under review explored this vascular link in depth through a double-blind, randomized, placebo-controlled trial examining whether tadalafil, a phosphodiesterase type 5 (PDE5) inhibitor, could improve endothelial function in men with erectile dysfunction — not merely by symptom relief but through measurable endothelial repair. The findings reposition tadalafil as more than a facilitator of sexual performance; it emerges as a therapeutic adjunct in vascular health, potentially bridging the gap between cardiology and sexual medicine.
Understanding Endothelial Dysfunction: The Common Denominator
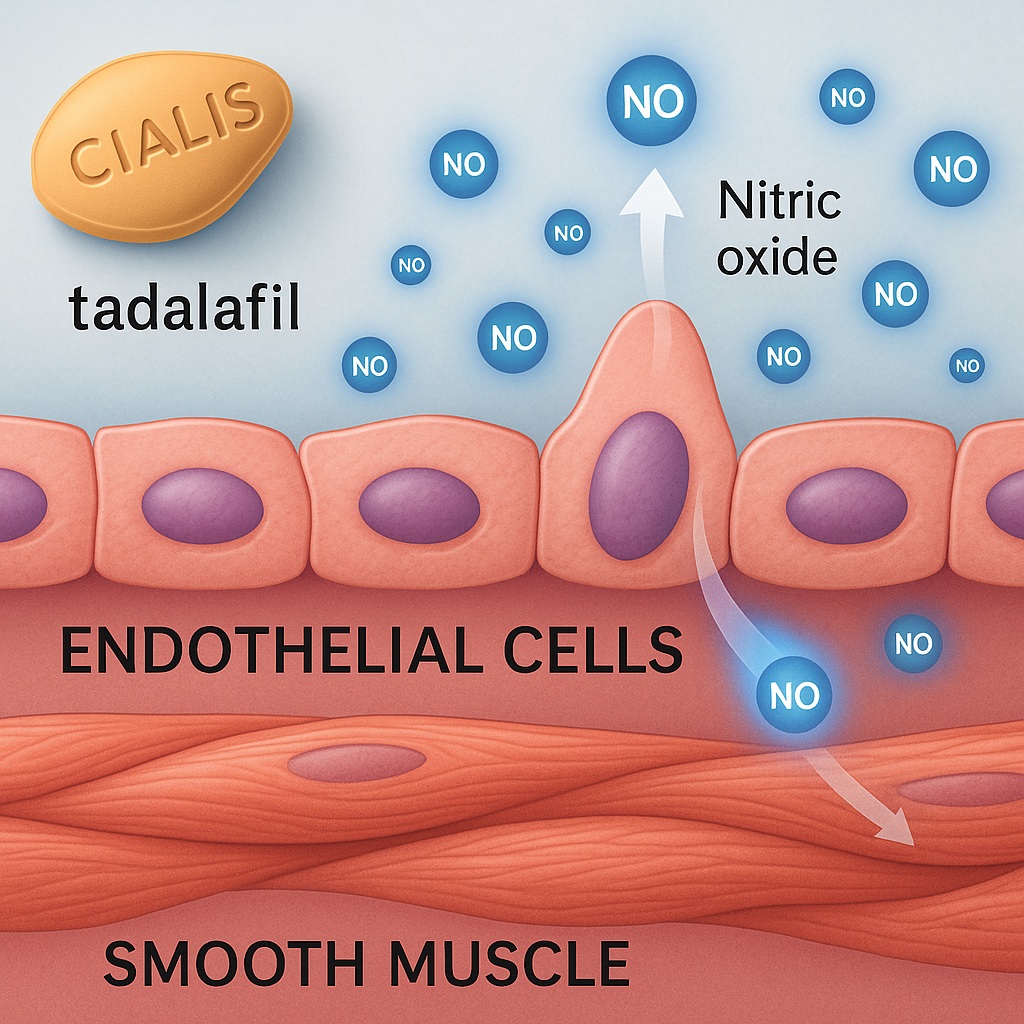
Endothelial dysfunction represents a state of impaired vasodilation, increased oxidative stress, and inflammatory activation. Normally, the endothelium synthesizes nitric oxide (NO) via endothelial nitric oxide synthase (eNOS), which diffuses to smooth muscle cells, increasing cyclic guanosine monophosphate (cGMP) levels, thereby inducing relaxation and vascular dilation. This same NO–cGMP cascade underpins penile erection.
When endothelial cells are exposed to metabolic or mechanical stressors — hyperglycemia, dyslipidemia, hypertension, or smoking — NO bioavailability diminishes. This imbalance tips the vascular system toward constriction, thrombosis, and inflammation. Not surprisingly, this dysfunction manifests both as coronary microvascular disease and erectile insufficiency. Indeed, ED has been described as a “penile angina”, often preceding coronary artery disease by several years.
In this context, assessing endothelial health in patients with ED offers a window into systemic vascular integrity. Therapies that restore endothelial function, therefore, hold dual significance: they may alleviate ED and simultaneously mitigate cardiovascular risk.
Tadalafil: A Pharmacologic Synopsis
Tadalafil belongs to the family of PDE5 inhibitors, alongside sildenafil and vardenafil, but distinguishes itself through its pharmacokinetic profile. Its half-life of approximately 17.5 hours supports prolonged plasma exposure, allowing for once-daily dosing and sustained endothelial effects. Unlike on-demand regimens, continuous administration of tadalafil maintains steady cGMP levels, fostering endothelial repair over time.
Mechanistically, PDE5 inhibitors prevent the degradation of cGMP, potentiating the downstream effects of NO signaling. However, beyond their acute vasodilatory action, mounting evidence suggests they enhance endothelial regeneration, reduce oxidative stress, and improve microvascular flow. These pleiotropic effects justify exploring tadalafil as a chronic endothelial therapy rather than a transient symptomatic remedy.
Study Design and Methodology: Scientific Rigor in Action
The trial was meticulously structured as a double-blind, randomized, placebo-controlled study, enrolling men aged 35–65 years with clinically diagnosed erectile dysfunction of vascular origin. Patients with significant cardiac disease, hormonal abnormalities, or psychological causes were excluded to isolate endothelial pathology as the primary driver.
Participants were randomly assigned to receive tadalafil 20 mg daily or placebo for a defined treatment period. Endothelial function was assessed using flow-mediated dilation (FMD) of the brachial artery, a validated surrogate marker for systemic endothelial performance. Measurements were obtained at baseline and post-treatment, alongside assessments of sexual function scores, lipid profiles, and inflammatory biomarkers such as high-sensitivity C-reactive protein (hsCRP).
This methodological rigor ensured that the trial could not only quantify erectile improvement but also determine whether tadalafil exerted systemic vascular benefits independent of sexual activity.
Baseline Characteristics: A Profile of Cardiometabolic Risk
The participants reflected a familiar clinical portrait: men with mild to moderate ED accompanied by varying degrees of cardiometabolic risk. Many exhibited elevated fasting glucose, borderline hypertension, or subclinical dyslipidemia — hallmarks of early endothelial decline. Importantly, none had overt cardiovascular disease, aligning with the hypothesis that ED often predates macrovascular complications.
By focusing on this intermediate-risk population, the investigators targeted the “silent” phase of vascular disease — where endothelial dysfunction is reversible and therapeutic intervention could yield both functional and prognostic dividends.
Key Findings: Restoration of Endothelial Function
The results were striking in both statistical and physiological terms. After several weeks of daily tadalafil administration, flow-mediated dilation increased significantly compared to placebo. This improvement reflected a direct enhancement in endothelial-dependent vasodilation, indicating restored NO bioactivity. Notably, these vascular benefits persisted even after controlling for confounding factors such as age, baseline FMD, and metabolic parameters.
Parallel improvements were observed in erectile function scores, confirming that symptomatic relief correlated with objective vascular recovery. The dual restoration of endothelial and erectile function strengthened the argument that tadalafil’s benefits stem from fundamental vascular repair rather than isolated penile hemodynamics.
Moreover, hsCRP levels declined modestly, suggesting a reduction in systemic inflammation — an encouraging signal that PDE5 inhibition might attenuate the inflammatory milieu fueling endothelial injury.
Mechanistic Insights: From the Molecule to the Microvasculature
How does tadalafil repair the endothelium? The answer lies in its ability to amplify NO signaling and counteract oxidative stress. By inhibiting PDE5, tadalafil prevents cGMP degradation, thereby maintaining smooth muscle relaxation and shear stress — key stimuli for endothelial health. This sustained shear stress upregulates eNOS expression, establishing a positive feedback loop of NO synthesis and vascular compliance.
Furthermore, chronic PDE5 inhibition has been shown to suppress NADPH oxidase activity, lowering reactive oxygen species (ROS) generation. Reduced oxidative stress not only preserves NO bioavailability but also protects endothelial cells from apoptosis and inflammatory activation. The resulting environment fosters endothelial regeneration, aligning pharmacologic action with physiologic restoration.
These molecular dynamics echo those observed with statins and ACE inhibitors, placing tadalafil within a broader pharmacologic class of endothelial therapeutics rather than mere vasodilators.
Beyond the Penis: Systemic Vascular Implications
One of the most compelling aspects of this research is its implication that the benefits of tadalafil transcend erectile physiology. Improvements in brachial artery FMD imply a systemic endothelial response, potentially relevant to other vascular territories — including the coronary and cerebral circulations.
Endothelial repair mechanisms are inherently systemic: circulating progenitor cells, NO signaling, and inflammatory mediators affect multiple vascular beds. Therefore, a therapy that normalizes endothelial function in the penile vasculature may concurrently improve arterial elasticity, reduce atherogenesis, and enhance overall cardiovascular health.
This concept redefines the PDE5 inhibitor class. Rather than being confined to the treatment of erectile dysfunction or pulmonary hypertension, agents like tadalafil may soon occupy a therapeutic niche in endothelial dysfunction syndromes, spanning from diabetic vasculopathy to early atherosclerosis.
Clinical Interpretation: Reassessing the Therapeutic Hierarchy
In clinical practice, erectile dysfunction is often managed symptomatically, with PDE5 inhibitors prescribed as needed for sexual activity. This study compels clinicians to reconsider such intermittent dosing, advocating instead for chronic administration in select patients to leverage tadalafil’s endothelial benefits.
For men with both ED and early markers of cardiometabolic risk — prediabetes, hypertension, dyslipidemia — daily tadalafil may serve a dual function: improving sexual performance and stabilizing vascular health. This approach aligns with the modern concept of vascular continuum management, where treating one manifestation (ED) concurrently mitigates systemic disease progression.
Moreover, the safety profile observed in this study reinforces the feasibility of such long-term use. Adverse effects, primarily mild headache and flushing, were transient and self-limiting, reflecting tadalafil’s well-established tolerability.
Comparative Perspective: Tadalafil Versus Other PDE5 Inhibitors
While sildenafil and vardenafil share the same pharmacologic target, tadalafil’s prolonged half-life confers a distinct clinical advantage for endothelial therapy. Continuous exposure ensures sustained PDE5 inhibition, maintaining basal NO-cGMP signaling and endothelial conditioning. This contrasts with the short-acting PDE5 inhibitors, whose intermittent effects may be insufficient to induce vascular remodeling.
Additionally, tadalafil demonstrates less cross-reactivity with other phosphodiesterase isoforms, minimizing systemic adverse events such as visual disturbances linked to PDE6 inhibition. Its predictable pharmacokinetics and minimal food interactions further enhance its suitability for chronic use.
Thus, among its pharmacologic peers, tadalafil emerges as the most viable candidate for repositioning as an endothelial health agent rather than an episodic performance enhancer.
Integrating the Evidence: A New Paradigm in Sexual and Vascular Medicine
The cumulative evidence from this and related studies suggests a paradigm shift: erectile dysfunction should be approached as an endothelial disorder first, a sexual disorder second. In this framework, PDE5 inhibitors like tadalafil are not only symptom relievers but vascular rehabilitators.
This reconceptualization carries profound implications for both urology and cardiology. For urologists, it broadens the therapeutic ambition from restoring erections to rejuvenating vascular health. For cardiologists, it underscores the diagnostic value of ED as a harbinger of endothelial dysfunction — a prompt to assess and intervene before overt cardiovascular disease emerges.
Such interdisciplinary synthesis could transform preventive medicine, merging sexual health and vascular wellness under the shared banner of endothelial restoration.
Limitations and Scientific Reflection
No clinical study is without caveats. The trial’s sample size was modest, limiting generalizability. The duration of therapy was also relatively short, leaving open questions about the long-term sustainability of endothelial improvements. Moreover, while FMD is a validated marker, it remains a surrogate endpoint rather than a direct measure of clinical cardiovascular benefit.
Additionally, the study population comprised men with predominantly mild-to-moderate ED. Whether tadalafil exerts similar vascular benefits in severe or secondary ED (e.g., post-prostatectomy, diabetes) remains to be established.
Nevertheless, these limitations do not diminish the trial’s conceptual impact. It provides a biologically plausible, clinically relevant foundation upon which larger and longer studies can build.
Future Directions: Tadalafil in the Era of Vascular Precision Medicine
The intersection of sexual and cardiovascular health represents fertile ground for precision medicine. Future research should explore:
- Long-term endothelial remodeling: Whether chronic tadalafil use can reduce cardiovascular events in high-risk populations.
- Biomarker integration: Identifying molecular signatures (e.g., eNOS phosphorylation, NO metabolites) that predict response.
- Combination therapies: Assessing synergy with statins, SGLT2 inhibitors, or anti-inflammatory agents in endothelial restoration.
- Gender and age expansion: Investigating potential benefits in postmenopausal vascular dysfunction, where NO signaling also declines.
Ultimately, the goal is to reposition tadalafil not just as a symptomatic therapy but as part of a vascular health continuum, linking sexual function to systemic endothelial resilience.
Conclusion: Tadalafil as an Endothelial Therapeutic Frontier
The trial’s findings invite a reimagining of tadalafil’s role in medicine. Beyond facilitating erections, tadalafil acts as a pharmacologic architect of endothelial repair — restoring NO balance, improving vascular tone, and dampening inflammation. In doing so, it bridges disciplines, connecting sexual health with cardiovascular preservation.
The implications extend beyond men with erectile dysfunction. They touch upon the broader narrative of vascular aging, microcirculatory decline, and the silent erosion of endothelial integrity that precedes much of modern chronic disease. Tadalafil, by enhancing endothelial performance, may yet redefine the therapeutic approach to vascular wellness itself.
FAQ
1. Does tadalafil truly improve vascular health beyond treating erectile dysfunction?
Yes. Clinical and mechanistic studies demonstrate that tadalafil enhances endothelial function systemically by restoring nitric oxide–cGMP signaling, improving flow-mediated dilation, and reducing oxidative stress. These effects extend beyond the penile vasculature to broader cardiovascular health.
2. How does tadalafil differ from sildenafil in endothelial benefits?
While both inhibit PDE5, tadalafil’s longer half-life allows continuous endothelial conditioning, producing more stable improvements in vascular reactivity. Its favorable safety and pharmacokinetic profiles make it better suited for chronic administration.
3. Can tadalafil prevent cardiovascular disease in men with ED?
While this remains an active area of research, current evidence suggests that improving endothelial function with tadalafil could reduce cardiovascular risk over time. Large-scale longitudinal studies are needed to confirm whether this translates into lower rates of major adverse cardiac events.
